Prostate Cancer - PI-RADS v2.1
Georgios Agrotis¹, Rhiannon van Loenhout², Frank Zijta², Robin Smithuis³ and Ivo Schoots⁴
¹Radiology Department of University Hospital of Larissa in Greece and ²the Haaglanden MC, ³Alrijne Hospital and ⁴Erasmus MC in the Netherlands
Publicationdate
The introduction of the Prostate Imaging–Reporting and Data System (PI-RADS) classification in 2012 significantly improved the standardization of acquisition, interpretation, and reporting of multiparametric MRI (mpMRI) of the prostate.
The PI-RADS Steering Committee has since proposed several refinements to PI-RADS Version 2.0, resulting in the updated PI-RADS Version 2.1.
Modifications in PI-RADS v2.1 Include:
- Refinements in the acquisition plane of T2W imaging.
- Updated recommendations for DWI b-value usage and DCE-MRI temporal resolution.
- Revised criteria for interpretation of DWI and DCE, including clarification on the role of biparametric MRI (bpMRI).
- Special considerations for lesions located in the anterior fibromuscular stroma (AFMS) and central zone (CZ).
- Enhanced evaluation criteria for PI-RADS category 2 lesions in the transition zone (TZ), including guidance for background signal assessment.
Modifications to the version 2.0 will be highlighted.
Introduction

The PI-RADS assessment categories are based on the findings of multiparametric MRI, which is a combination of T2-weighted (T2W), diffusion weighted imaging (DWI) and dynamic contrast-enhanced (DCE) imaging.
It is an accurate tool in the detection of clinically significant prostate cancer.
In PI-RADS v2.1 clinically significant cancer is defined on pathology as:
- Gleason score ≥ 7 - including 3+4 with prominent but not predominant Gleason 4 component and/or
- Tumor volume > 0.5cc and/or
- Extraprostatic extension (EPE).
Gleason score
The Gleason score is used by pathologists to grade prostate cancers.
If the cancer cells and their growth patterns look very abnormal, a grade 5 is assigned. The Gleason score is the sum of the two most prevalent patterns.
These 2 grades are added to yield the Gleason score.
The highest Gleason score therefore is 10.
For example, if the Gleason score is written as 3+4=7, it means that most of the tumor is grade 3 and the second most common or most malignant grade is 4.

PI-RADS version 2.1
The table is based on the PI-RADS version 2.1.
Changes from the old version 2.0 are indicated in light red.
Assessment by Zonal Anatomy
Correct identification of the anatomic zone (Peripheral Zone vs Transition Zone) is critical, as the dominant sequence used to determine PI-RADS score varies by location.
Peripheral zone (PZ)
The peripheral zone is situated on
the posterior and lateral side of the prostate, surrounding the transition
zone.
In the Peripheral Zone, DWI/ADC is the dominant sequence.
- Lesions scored PI-RADS 3 based on DWI/ADC:
- Remain PI-RADS 3 if DCE is negative
- Are upgraded to PI-RADS 4 if DCE is positive (i.e., early focal enhancement)
Updates in PI-RADS v2.1:
- There is a more precise description of peripheral zone lesions in PI-RADS category 2 and 3.
Transition zone (TZ)
The transition zone surrounds the
prostatic urethra and enlarges in aging men as a result of benign prostatic
hyperplasia.
In the Transition Zone, T2-weighted imaging is the dominant sequence.
PI-RADS Category Adjustment Based on DWI/ADC:
- A T2W score 2 lesion:
- Remains PI-RADS 2 if DWI/ADC ≤ 3
- Becomes PI-RADS 3 if DWI/ADC ≥ 4
- A T2W score 3 lesion:
- Remains PI-RADS 3 if DWI/ADC < 5
- Becomes PI-RADS 4 if DWI/ADC = 5
Updates in PI-RADS v2.1:
- Round, fully encapsulated nodules are now assigned PI-RADS 1.
- More precise criteria for category 2 lesions.

Peripheral zone (PZ)
A lesion assessed as suspicion category 3 based on DWI/ADC, remains a PI-RADS score 3 if there is no focal enhancement (negative), however, it becomes a PI-RADS score 4 if there is focal enhancement (positive).
Transition zone (TZ)
A lesion assessed as category 2 based on T2W images remains PI-RADS score 2 if the DWI/ADC is ≤ 3, however it becomes PI-RADS score 3 if the DWI is ≥ 4.
A lesion assessed as category 3 based on T2w images remains PI-RADS score 3 if the DWI is ≤ 4, however, it becomes a PI-RADS score 4 if the DWI/ADC is score 5.
Peripheral zone

PI-RADS
For the peripheral zone the DWI/ADC is the primary determining sequence to assign the PI-RADS assessment category.
Peripheral zone - DWI/ADC category 1
- No abnormality visible on ADC and high b-value DWI.

Peripheral zone - DWI/ADC category 2
- Linear/wedge shaped configurations with hypointensities on ADC and/or linear/wedge shaped hyperintensities on high b-value DWI.

Peripheral zone - DWI/ADC category 3
- Focal (discrete and different from the background) hypointensity on ADC and/or focal hyperintensities on high 3 b-value DWI
- May be markedly hypointensity on ADC or markedly hyperintensity on high b-value DWI, but not both.
- A category 3 lesion remains a PI-RADS score 3 if there is no focal enhancement (negative), but becomes a PI-RADS score 4 if the enhancement is focal.

Peripheral zone - DWI/ADC category 4
- Focal markedly hypointensity on ADC and markedly hyperintensity on high b-value DWI
- <1.5cm in greatest dimension.

Peripheral zone - DWI/ADC category 5
- Same as as assessment score 4 but ≥1.5cm in greatest dimension or
- Definite extraprostatic extension (EPE) or invasive behavior.

Examples of PI-RADS 1-5
Examples of PI-RADS scores 1-5 are given in the table.
In the peripheral zone, the PI-RADS assessment category of a lesion is determined primarily on DWI/ADC and correlated to T2W- and DCE-images.
In the peripheral zone an equivocal or indeterminate lesion (category 3) is assigned to PI-RADS category 4 if DCE is positive, i.e focal or earlier contrast enhancement.
The lesion remains assigned to PI-RADS category 3 if the DCE is negative, i.e. no early enhancement or diffuse enhancement and not corresponding to the focal T2W/DWI lesion or focal enhancement corresponding to BPH.

Prostate cancer in PZ
For the peripheral zone the DWI/ADC is the primary determining sequence to assign the PI-RADS assessment category.
First look at the images and describe what you see.
A 16 mm lesion (measurement not
shown) was detected and located dorsally in the peripheral zone of the
mid-portion of the prostate on the right.
This lesion was assigned to PI-RADS
category 5, based on marked hypointensity on ADC and marked hyperintensity on
DWI (score 5 - dominant sequence), correlated to markedly hypointensity on T2W
(score 5).
The Gleason score was 3+4, which
means intermediate risk of an aggressive cancer.
The lesion does not abut the
pseudocapsule and there is no sign of extraprostatic growth.
Suspicious lesions in the peripheral zone typically have the following characteristics on T2W-images:
- ill-defined
- hypointense signal on ADC and T2w images
Less suspicious features are the following characteristics on T2W-images:
- bilateral
- symmetry
- diffusely distributed signal changes
- wedge shaped
- sharply demarcated foci of hypointensity

First look at the images and then continue reading.
The findings are:
- A 17 mm lesion (measurement not shown) is located in the peripheral zone, dorsally on the left in the mid-portion of the prostate.
- It is markedly hypointense on ADC, and markedly hyperintens on DWI.
- It corresponds to a hypointense area on T2W.
- On T2W there is broad-based contact with the capsula.
This lesion was assigned to PI-RADS
category 5 with suspicion of extraprostatic extension.
The Gleason score was 4+3.
This suspected lesion has significant
diffusion restriction .
The ADC measured 440 mm2/s.
Low ADC values indicate a higher risk
of malignancy.
The actual ADC value is inversely
correlated to the likelihood of a clinically significant malignancy.
Values above 900 mm2/s are considered
likely benign and below 750 mm2/s likely malignant.
However quantification results may
vary substantially between scanners and protocols.

First look at the images and then continue reading.
The findings are:
- A lesion with PI-RADS assessment category 4 located in the left
peripheral zone in the mid-portion of the prostate.
Focal marked hypointensity on ADC (yellow arrow) (score 4), corresponding an hypointense area on T2W (score 4).
The Gleason score of this lesion was 3+4.
- A lesion with PI-RADS assessment category 3 is located in the right peripheral zone, with mild focal hypointensity on ADC (green arrow) with isointensity on DWI (score 3).
No DCE was performed and no further
discrimination could be determined.
Biopsy did not show any sign of
malignancy.
Transition Zone
PI-RADS
Transitional zone - T2W category 1
- Normal appearing TZ (rare) or
- Round completely encapsulated nodule (“typical nodule”)
Transitional zone - T2W category 2
- Mostly encapsulated nodule or
- Homogeneous circumscribed nodule without encapsulation. (“atypical nodule”) or
- Homogeneous mildly hypointense area between nodules
- If the DWI has a score 4 or more, then the lesion is categorized as
PI-RADS category 3.
Transitional zone - T2W category 3
- Heterogeneous signal intensity with obscured margins
- Includes others that do not qualify as 2, 4, or 5
- If the DWI has a score of <4, then the lesion is categorized as PI-RADS score 3.
- If the DWI has a score of 5, then the lesion is categorized as PI-RADS score 4.
Transitional zone - T2W category 4
- Lenticular or non-circumscribed, homogeneous, moderately hypointense,
- and <1.5 cm in greatest dimension
Transitional zone - T2W category 5
- Same as score 4, but ≥1.5cm in greatest dimension or
- Definite extraprostatic extension or invasive behavior

Examples of PI-RADS 1-5
In the transition zone, the PI-RADS assessment category of a lesion is determined primarily on T2W-images and then correlated to DWI/ADC.
Examples of PI-RADS categories 1-2 are given in the table.
Click to enlarge the image.

In the transition zone an equivocal or indeterminate lesion (category 3) is assigned to PI-RADS category 4 if the DWI corresponds with score 5 (markedly intense greater than 1.5cm).
The lesion remains assigned to PI-RADS category 3 if the DWI corresponds to DWI score 4 (markedly intense but less than 1.5cm) or a lower score.
Examples of PI-RADS categories 3-5 are given in the table.
Click to enlarge the image.

Prostate cancer in TZ
Suspicious lesions typically have the following characteristics:
- non-circumscribed
- homogeneous
- relatively hypointense
- smudged appearance on T2W images, sometimes mentioned as "erased charcoal" appearance.
- lenticular or droplet-like shape
- spiculated margins.
Images
There is a lesion in the right anterior part of the transition zone.
It has irregular margins on T2W images (score 4) and is focal markedly hypointense on ADC (680 mm/s) (score 4), not exceeding 15 mm in length.
This lesion corresponds to a PI-RADS category 4.
MR-Ultrasound fusion-guided biopsy resulted in a Gleason 3+4.
In the right peripheral zone there is a wedge-shaped slightly hypo-intense area (score 2) without suspicious chracteristics on DWI/ADC (score 2).
It was assigned as PIRADS category 2.This region is benign and has
most likely glandular atrophy or focal inflammatory findings on histopathology.

High-grade tumors often reveal a
lower T2W signal intensity than low-grade tumors.
Extension into the anterior
fibromuscular stroma or the urethral sphincter can be seen.
In general, suspicious lesions in the
transition zone are frequently challenging to distinguish from the surrounding
hyperintense glandular and hypointense stromal tissue.
Images
There is a lesion located anteriorly in the midline, most likely in the anterior fibromuscular stroma at the junction of the base and the mid-portion of the prostate.
There is no extraprostatic extension.
The lesion has irregular margins on T2W images with an
"erased charcoal" appearance, exceeding 15 mm in maximum length (score
5) and is markedly hypointense on ADC (score 5).
Category: PI-RADS 5.
MR/Ultrasound fusion-guided biopsy resulted in a Gleason
3+4.

Images
27mm lesion anterior in the apex of
the transition zone, with an "erased charcoal" appearance.
This corresponds to an area of
restricted diffusion with a droplet-shape.
The lesion was scored a PIRADS category
5.
MR/Ultrasound fusion-guided biopsy
resulted in a Gleason 3+4.
Anterior Fibromuscular Stroma

The normal AFMS shows bilaterally symmetric shape (“crescentic”) and symmetric low signal intensity similar to that of the obturator or pelvic floor muscles on T2W, ADC, and high b-value DWI without early enhancement.
Since prostate cancer does not originate from the AFMS, when reporting a suspicious lesion in the AFMS, criteria for either the PZ or TZ should be applied, depending on the zone from which the lesion appears most likely to be originating.

This is an example of an adenocarcinoma involving the AFMS.
Images
T2W: The left anterior TZ zone shows a lenticular
hypointense lesion.
A focal markedly hyperintense region on DWI corresponds to
hypointense focal markedly area on ADC.
DCE: The region of interest shows early
enhancement.
PI-RADS score: 4.
Histopathology: Gleason score 4+4 following
MRI fusion-guided targeted biopsy.
TNM-stage

TNM-staging is based on clinical (c) and pathological (p) findings, and if indicated on additional imaging findings.
For T-staging a prostate MRI is advised in:
- intermediate-risk prostate cancer (predominantly Gleason 4 pattern = ISUP ≥3)
- high-risk localized prostate cancer
- locally advanced prostate cancer
Nowadays there is increased utilization of prostate MRI in the primary diagnostic work-up.
The table only shows the stages that are relevant for imaging.
The full table is found here
 Poorly differentiated adenocarcinoma of the prostate
Poorly differentiated adenocarcinoma of the prostate
Locally advanced prostate cancer
The prostate does not have a true capsule.
However on MRI the outer border of the prostate does have a thin, hypointense line, which is histopathologically composed of a fibromuscular band.
This hypointense line can be used to assess extraprostatic tumor growth.
The neurovascular bundles are located at the posterolateral aspect of the prostate (at the 5 and 7 o'clock position, see example on the left).
Involvement of the neurovascular bundle should be specifically reported, as nerve-sparing surgery will not be possible.
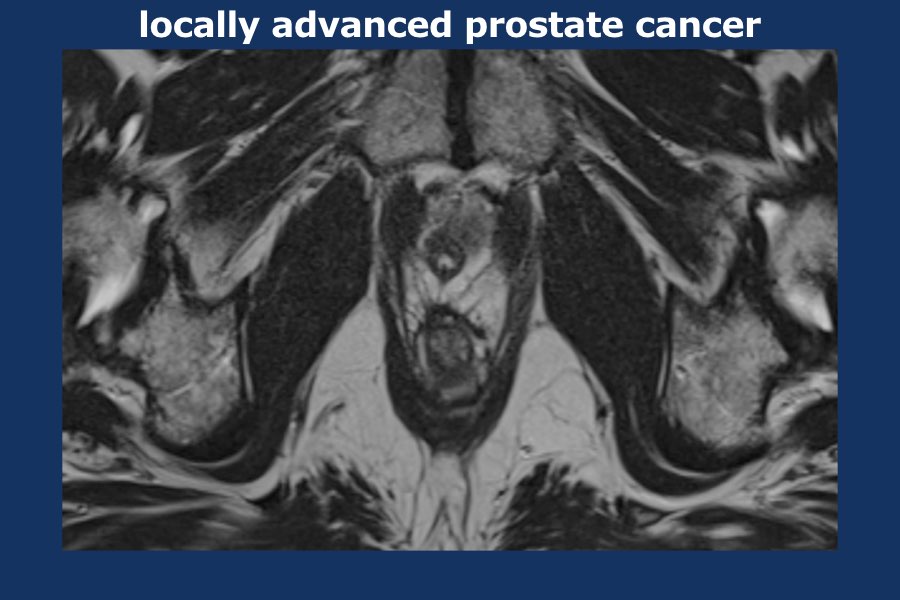
Scroll through the images of locally advanced prostate cancer.
There is a large lobulated tumor originating from the left prostate lobe infiltrating the mesorectum, the rectum as well as the left pelvic wall (i.e. T4).
There are large para-iliac and mesorectal lymphnodes distributed mainly on the left side of the pelvis (i.e. at least N1).
Left prostate needle biopsies proved localization of adenocarcinoma of the prostate.
Gleason score 9 (5 +4), volume percentage estimated 90%.

The vascular insertion at both the base and apex are susceptible locations for extraprostatic extension.
Seminal vesicle invasion can be observed by direct tumor extension into the vesicles.
Expansion of the vesicles, focal or diffuse low T2W signal intensity, abnormal contrast enhancement or restricted diffusion can also be features of involvement.
In addition, involvement is likely present when the angle between the prostate base and the vesicle is obliterated.
When the external urethra is involved at the apex, surgical excision can cause sphincter malfunction, resulting in incontinence.
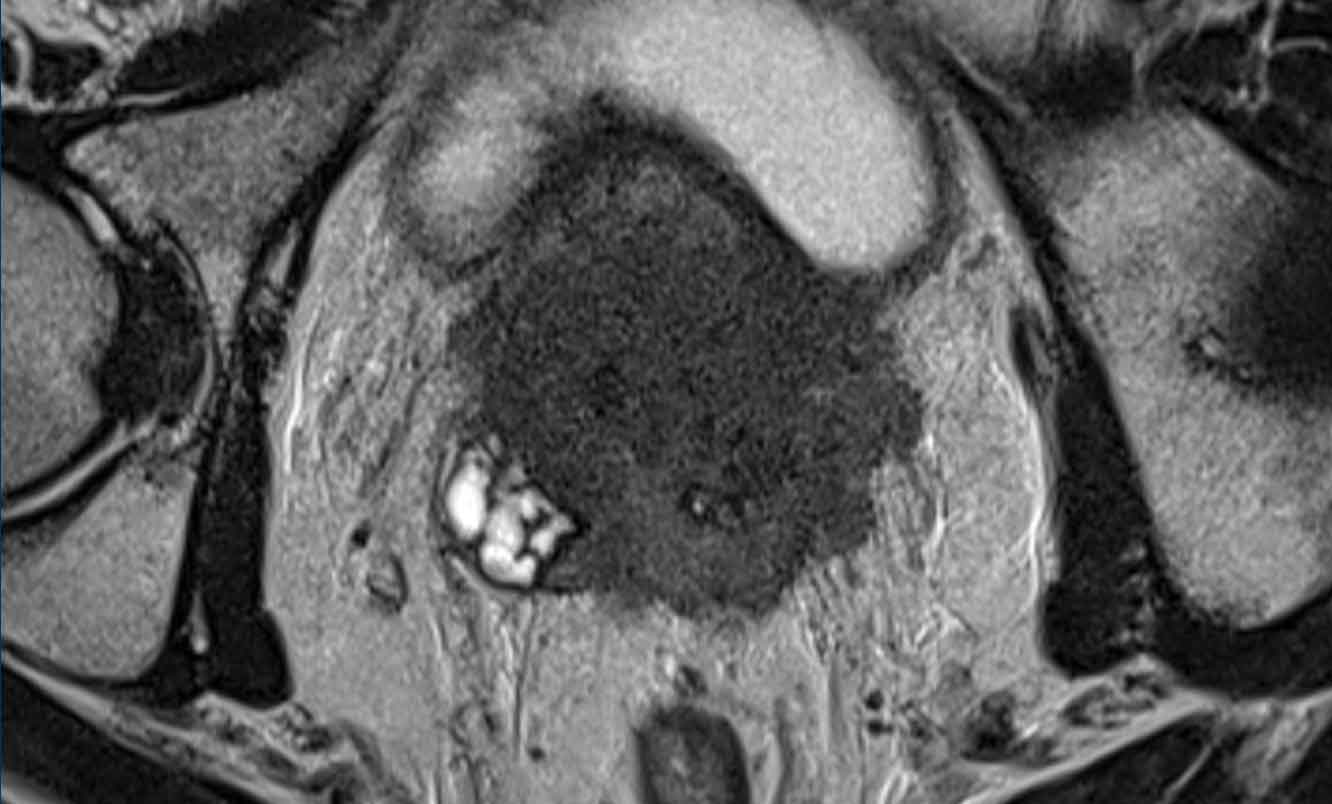
Images
The axial T2W-image at the level of the prostate base demonstrates low signal intensity replacing the normal signal intensity of the left peripheral zone, with direct tumor extension from the base of the prostate into both seminal vesicles (arrow).
Restricted diffusion appears as an area of low signal intensity on the ADC map.
Gleason score: 4+3.

N-stage
DWI is the best sequence for detection of lymph nodes.
T1W series are useful for interpretation of the border contour and signal characteristics of lymph nodes.
MR has a low accuracy for distinguishing positive or negative lymph nodes if characterization is based on size alone.
The following characteristics are considered suspicious:
- round shape and short axis of ≥8mm
- oval shape and short axis of ≥10mm
- heterogeneous appearance
- irregular margins
Regional lymph nodes (green) are below the level of the common iliac junction and are staged N1:
- pelvic
- hypogastric
- sacral
- iliac (internal, external)
Distant lymph nodes (red) are outside these regions and are staged as metastatic disease M1a:
- aortic
- common iliac
- inguinal
- supraclavicular
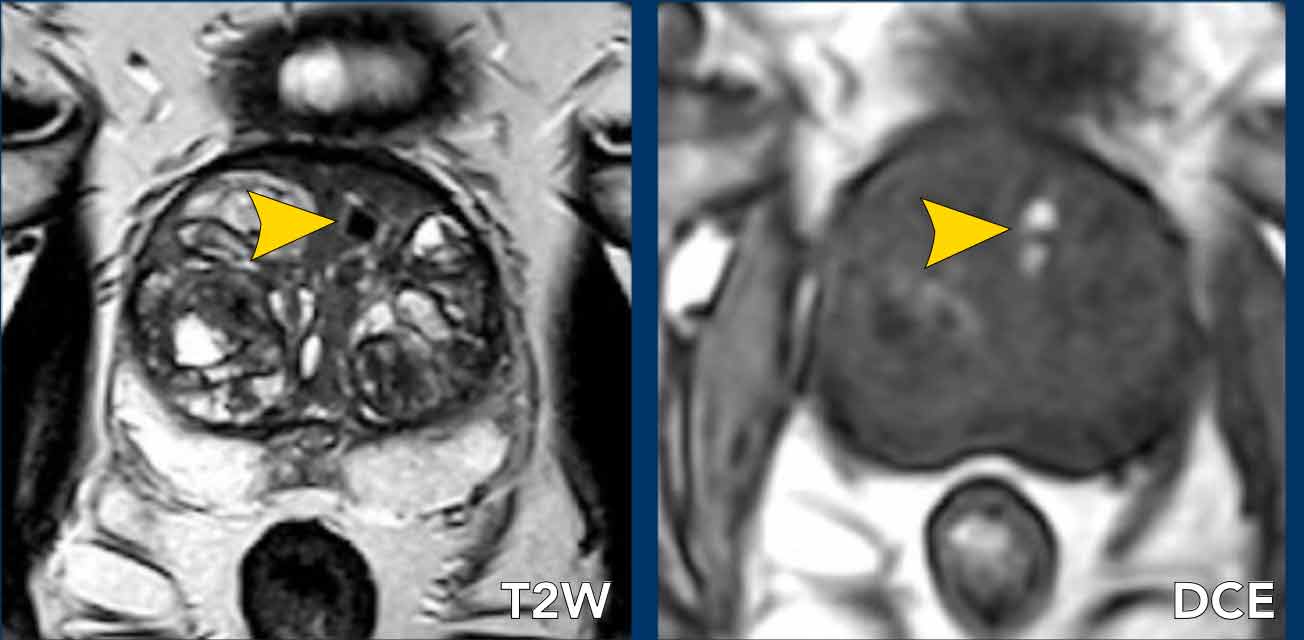
Benign findings

Benign prostate hyperplasia
Benign prostate hyperplasia (BPH) results in the formation of well-circumscribed, encapsulated nodules in the transition zone.
Some of these nodules have dense stroma with low T2W signal intensity and low ADC (yellow arrow).
The most important characteristic feature to distinguish BPH nodules from malignancy is the generally well-defined and well-circumscribed morphology interpreted in axial, coronal and sagittal series.
The left peripheral zone lesion was classified as PI-RADS 5 (red arrow).
MRI- targeted biopsy revealed a Gleason 3+4.

T2 hypointense BPH nodules can be less distinctly circumscribed within the transition zone and may show some degree of restricted diffusion.
Also, these nodules tend to enhance early and intensely on DCE, making conclusive characterization difficult.
Here a patient with BPH in the transition zone seen as heterogenous stroma with a large cystic area (arrow).
Biopsies showed chronic benign prostatitis.

Not all nodules exist in the transition zone.
Some can be ectopic and may be found in the peripheral zone (arrow).
This entity shouldn’t be confused with prostate cancer.

BPH consists of a mixture of stromal and glandular hyperplasia and may appear as band-like areas and/or encapsulated round nodules with circumscribed or encapsulated margins.
Image
This coronal T2W
image shows various types of BPH nodules.
- glandular nodule (blue circle)
- atypical nodule (yellow circle)
- nodule in nodule (various smaller nodules inside contained in a larger nodule) (green circle).

Predominantly glandular BPH nodules and cystic atrophy exhibit moderate-marked T2 hyperintensity and are distinguished from malignant tumors by their signal and capsule.
Image
Axial T2W image shows
a glandular BPH nodule with hyperintensity on T2W image surrounded by a
capsule.

Prostatitis
Prostatitis or rather inflammation is
a common finding in men and can occur in the absense of any clinical history or
symptoms.
Prostatitis and other benign features
like glandular fibrosis, scarring, atrophy and post-biopsy hemorrhage can mimic
prostate cancer in the peripheral zone, since all present as a focus of low
signal on ADC.
However benign features mostly
presents as a band-like or wedge-shaped or diffuse area of low signal
intensity, while prostate cancer is more round or droplet-shaped.
The hypointensity on ADC in inflammatory
prostatic tissue is usually not accompanied by hyperintensity on high b-value
DWI series.
Also ADC values in prostate cancer
tend to be lower than ADC levels in prostatitis.
On DCE there is increased
enhancement, which is therefore not helpful in the differentiation.
In case of chronic inflammation,
concordant fibrosis and focal atrophy may be observed, which presents as focal
retraction in the normal anatomic convexity of the peripheral zone.
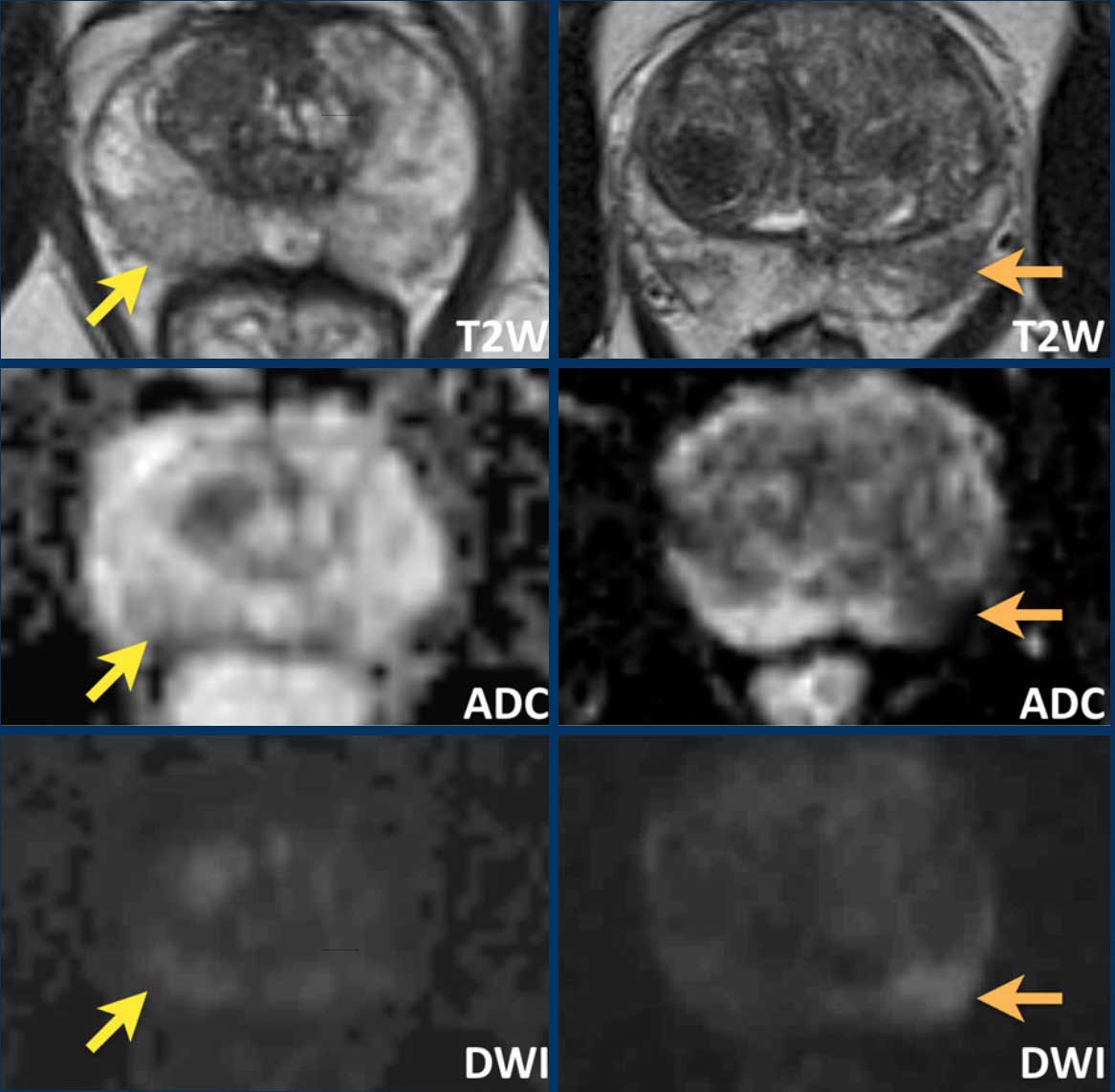 Differences between prostatitis ( images on the left) and prostate cancer (images on the right)
Differences between prostatitis ( images on the left) and prostate cancer (images on the right)
Here we see the differences between prostatitis ( images on the left) and prostate cancer (images on the right).
Left
The images on the left show a wedge-shaped area of mild hypointensity on T2W and ADC with no concordant high signal on DWI located dorsally in the right peripheral zone of the midportion of the prostate (yellow arrow).
This was interpreted as focal inflammation (PI-RADS category 2).
No biopsy performed.
Right
The images on the right show a clinically significant prostate cancer with an ill-defined zone of markedly hypointensity on T2W and ADC and focal high signal intensity on DWI dorsally in the left peripheral zone (PI-RADS category 4).
MRI-targeted biopsies showed a Gleason score of 4+3.

The images show bilateral wedge-shaped, sharply demarcated hypointense lesions in the peripheral zone with minimal low ADC signal.
These findings can be regarded as benign characteristics, i.e. inflammation.
Biopsies showed focally some inflammation with glandular hyperplasia.

The T2W-images show a diffusely
hypointense peripheral zone.
The ADC does not show any foci of
significant low signal intensity.
The DWI is hyperintense on both
sides.
The ADC value was 830 mm2/s.
This was interpreted as benign characteristics (PI-RADS category 2) and diagnosed as chronic inflammation.
Biopsies showed focal chronic active prostatitis and no malignancy.

A 70-year old patient was referred with a raised PSA of 9ng/ml, a PSA density 0.10.
A PI-RADS score of 5 was
given to a hypointense area in the right peripheral zone at the midgland, with
diffusion restriction (black arrow).
The DCE showed vivid and peripheral enhancement of the lesion (arrowheads).
A biopsy was performed and the histopathology results showed abscess formations.
Peripheral enhancement and diffusion restriction are typical imaging findings of an abscess.
 Hemorrhage. The DCE image is prior to contrast enhancement.
Hemorrhage. The DCE image is prior to contrast enhancement.
Hemorrhage
Hemorrhage in the peripheral zone and in the seminal vesicles is common after biopsy.
It appears as focal or diffuse hyperintense signal on T1W and iso- or hypointense signal on T2W.
However, chronic blood products may appear hypointense on all MR sequences.
This is a case of a 78-year old patient with raised PSA that underwent a prostate biopsy the previous year before undertaking one again.
Images
Hypointense lesions are seen on T2W in the anterior TZ zone.
These small lesions have high signal on T1W, indicating blood products.
No cancer was found after fusion-guided targeted biopsy.
Hemorrhage findings should always be reported.

Cysts
A variety of cysts can occur in the prostate and adjacent structures.
As elsewhere in the body, cysts in the prostate may contain “simple” fluid and appear markedly hyperintense on T2W and hypointense on T1W.
However, they can also contain blood products or proteinaceous fluid, which may demonstrate a variety of signal characteristics, including hyperintense signal on T1W.
Images
T2W
image shows a focal region of hyperintensity in the left peripheral zone of the
prostate.
This area corresponds to a hypointense area in DCE images (images
prior to enhancement).
Restricted
diffusion is present.
This corresponds to a proteinaceous cyst.
Prostate volume and PSA density

Prostate volume determines the feasibility of external radiation therapy, which can be performed up to a volume of 55cc.
Please note that this limit is only valid for conventional extern radiation.
For proton radiation this limit don't exist.
PSA density-values of ≥ 0,20 contribute towards the suspicion of a clinically significant prostate malignancy.

In this case the measurements of the prostate are 36 x 50 x 60mm (AP x LR x CC).
This results in a volume of 0,52 x (3,6 x 5,0 x 6,0) = 56,2 cc.
The PSA level in this patient was 5.
The PSA density is 5 : 56,2 = 0,09.
This is a low PSA density and this patient probably has no clinically significant malignancy.
Ellipsoid formulation:
Maximum AP and longitudinal diameters on a mid-sagittal T2W image and maximum transverse diameter on an axial T2W image multiplied by 0.52.
MR-protocol

In PI-RADS v2.1 the recommended sequences and settings are:
- T2WI
Axial plane is axial to the patient or in an oblique axial perpendicular to the long axis of the prostate. At least one additional orthogonal plane (sagittal and/or coronal). - DWI
ADC map calculation should be performed using a low b-value set at 0-100 sec/mm2 (with preference for 50-100 sec/mm2), an intermediate b-value set at 800-1000 sec/mm2, and optionally additional b-values in the range of 100-1000 sec/mm2.
A high b-value (≥1,400 sec/mm2) image set is also mandatory (preferably obtained from a separate acquisition or calculated from the low and intermediate b-value images). - DCE
Temporal resolution ≤15 seconds is advised and 3D T1W GRE is preferred.

Spasmolytic agents
Spasmolytic agents can be considered prior to examination to reduce movements of the small and large bowel.
Air and feces within the rectum can impair diffusion assessment.
The images are of a patient who did not receive any preparation prior to the MR-exam.
The presence of air and stool in the rectum induces discrete linear artifactual distortion in the region of the prostate, restricting the diagnostic accuracy of both the DWI and ADC series.

Here an example of a patient who did receive a minimal preparation enema administered a few hours prior to the exam.
This resulted in an evacuated rectum. Although an enema may induce rectal peristalsis, no artifacts were observed in this patient.

T1W
T1W-images determine the presence of post-biopsy hemorrhage.
This patient had systematic TRUS-guided biopsies 3 weeks earlier
Images
High signal
intensity on T1W image in the right peripheral zone, with little signal
reduction on T2W images, and no restricted diffusion on DWI / ADC (yellow
arrow).
Furthermore, a suspicious lesion was
identified right anteriorly in the transition zone with low signal intensity on
T2W and ADC and high signal intensity on DWI (black arrow).
This lesion showed a Gleason score 4+3 following MRI-targeted biopsy.

A large FOV up to the aortic bifurcation helps to assess extraperitoneal and pelvic lymph node involvement and osseous metastatic disease (arrow in figure).
T2W
High-resolution T2W FSE sequences are obtained in the axial and sagittal plane.
T2W images show anatomical information on normal and abnormal prostatic tissue.
Additional 3D T2 acquisitions can be used for reconstruction in all three anatomic planes and potential radiotherapeutic purposes.
The video nicely demonstrates the high resolution of the transverse 3D images with coronal and sagittal reconstructions.

DWI
Diffusion restriction is present when a lesion with high DWI signal corresponds to low signal on the ADC map, which is highly correlated to malignant cells.
The exact ADC value of the lesion is inversely correlated to the likelyhood of a malignant lesion.
High b-values are necessary to create a high signal-to-noise ratio.
B-value of at least 1400 is recommended.
Notice the difference between the B1000 and B1400 images.
A fusion guided biopsy of the lesion anterior in the prostate demonstrated a Gleason 3+4.
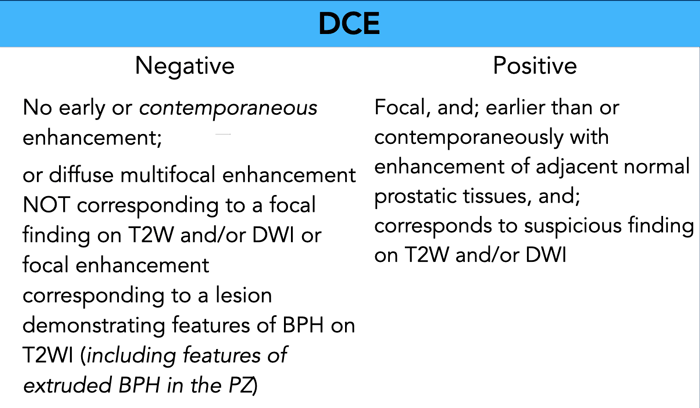 Modified criteria for a negative score on DCE in PI-RADS v2.1 are in italic. Criteria for a positive score on DCE remain unchanged.
Modified criteria for a negative score on DCE in PI-RADS v2.1 are in italic. Criteria for a positive score on DCE remain unchanged.
DCE
The criteria for a negative or positive dynamic contrast enhancement series are shown in the table.
DCE can be of additional value in confirming the suspicious conspicuity of a lesion, but are frequently non-specific as prostate cancer may reveal early and increased enhancement but also normal enhancement compared to normal prostate tissue.
Lack of enhancement does not exclude malignancy, and increased enhancement can be the result of acute or chronic inflammation.
The temporal resolution of ≤15 seconds is advised and 3D T1W GRE is preferred.
Timing of the examination
Post-biopsy changes, i.e. hemorrhage and inflammation, are usually located in the peripheral zone or the seminal vesicles.
These changes may adversely affect the interpretation of multiparametric MRI whereas signal intensities might be altered.
As these changes tend to diminish over time, an time interval of at least 6 weeks or longer between biopsy and MRI is recommended in the PIRADS guideline.
In current daily practice there is a tendency to perform multiparametric MRI before obtaining biopsies which consequently resolve this issue.
PI–RADS 2.1 Lexicon examples

Marked is defined as “a more pronounced signal change than any other focus in the same zone”.
Images
Marked signal change in a patient aged 69 years old showed a raised PSA
of 13.3ng/ml, PSA density 0.16.
A score of PI-RADS 5 was given due to a low
intensity area in the right peripheral zone of the midgland with
characteristics of extraprostatic extension.
There is marked restriction of
diffusion.
The diameter of the lesion is 1.7cm.
Biopsy was performed with fusion guided targeted mpMRI – TRUS method.
Histopathology results showed
adenocarcinoma of Gleason 8 (4+4) with extraprostatic extension.

Non-circumscribed
Non-circumscribed means
"Ill-defined”
Image
A non-circumscribed region (ill-defined)
shows restriction of diffusion corresponding to a PI-RADS 3 nodule.

Wedge in the peripheral zone is defined as “having the shape of a wedge, pie, or V shaped”

Focal is defined as “discrete and different from the background”.
Images
Focal lesion in a patient aged 79 years old.
Due to a raised PSA
of 6.4ng/ml, PSA density 0.05, mpMRI was followed and a score of PI-RADS 4 was
given due to a low intensity area in the right anterior TZ zone in the
midgland.
There is focal restriction of diffusion and the diameter of the
lesion was 1.2cm.
Biopsy was performed with the fusion guided targeted mpMRI – TRUS method that showed an adenocarcinoma of Gleason 9 (4+5)

Linear is defined as in a line or band-like shape.
Images
Linear configuration in the
left peripheral zone, corresponds to a PI-RADS 2 score.

Lenticular is defined as having the shape of a double-convex lens, crescentic.

Completely encapsulated nodule
Bounded by a distinct, uniform, smooth low-signal line (BPH nodule).
Completely encapsulated nodule is entirely surrounded by a smooth low-signal line in at least two imaging planes and is called a typical nodule.

Mostly encapsulated nodule
Almost completely or incompletely encapsulated nodule is not entirely surrounded by a smooth low-signal line (“atypical nodule”) “

Homogeneous mildly hypointense area between nodules
Images
Homogeneous mildly hypointense area (arrowheads) between nodules in
the TZ zone corresponds to a PI-RADS 2 score.

Heterogeneous signal intensity with obscured margins
This means “not clearly seen or easily distinguished “
Images
A heterogeneous signal intensity (green arrowheads) suggesting benign features
(T2W - score 2), however with possible obscured margins (T2W) with limited restricted diffusion
(DWI/ADC - score 3), corresponds to a sum PI-RADS 3 score.
Check list and Reporting

Reporting is done according to the checklist as shown in the table.
Before we start the interpretation of the MRI, we need to be informed about:
- Family history
- Digital rectal examination
- PSA level
- Prior biopsies (quantity, location, Gleason score)
- Prior therapy
In case of multiple suspicious findings, the index lesion is the lesion with the highest PI-RADS assessment category.