Ankle Fracture Mechanism and Radiography
Robin Smithuis
Radiology Department of the Rijnland Hospital, Leiderdorp, the Netherlands
Publicationdate
The ankle is the most frequently injured joint.
Management decisions are based on the interpretation of the AP and lateral X-rays.
In this article we will focus on:
- Trauma mechanism of ankle injuries
- Ottawa ankle rules
- Proper positioning of the ankle for radiography
Trauma mechanism in ankle injuries
Normal flexibility of the ankle
The ankle joint has to be flexible in order to deal with the enormous forces applied exerted on the talus within the ankle fork. .
The medial side of the joint is quite rigid because the medial malleolus - unlike the lateral malleolus - is attached to the tibia and the medial collateral ligaments are very strong.
On the lateral side there is a flexible support by the fibula, syndesmosis and lateral collateral ligaments.
This lateral complex allows the talus to move laterally and dorsally in exorotation during forward motion and subsequently pushes it back into its normal position.
The fibula has no weight-bearing function, but merely serves as a flexible lateral support.
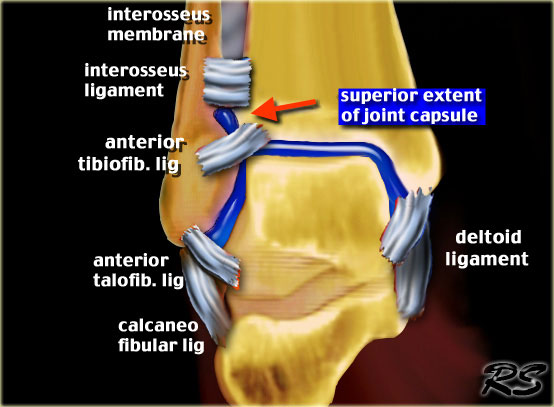
The syndesmosis is the fibrous connection between the fibula and tibia formed by the anterior and posterior tibiofibular ligaments - located at the level of the tibial plafond (French for ceiling) - and the interosseus ligament, which is the thickened lower portion of the interosseus membrane.
The anterior and posterior tibiofibular ligaments are often referred to as anterior and posterior syndesmosis.
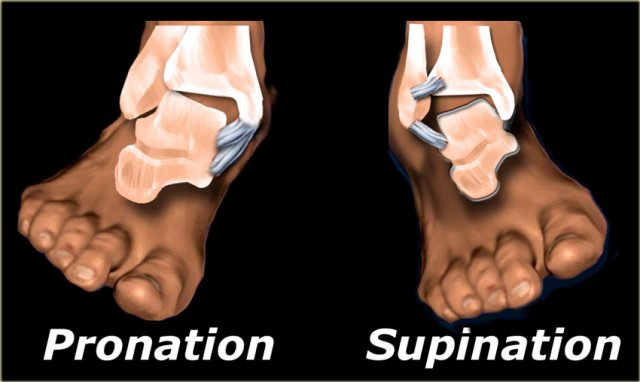
Vulnerable positions of the foot
There are two positions of the foot in which the flexible ankle joint becomes a rigid and vulnerable system: extreme supination and pronation.
In these positions forces applied to the talus within the ankle mortise can result in fractures of the malleoli and rupture of the ligaments.
In 80% of ankle fractures the foot is in supination.
The injury starts on the lateral side, since that is where the maximum tension is.
In 20% of fractures the foot is in pronation with maximum tension on the medial side.
The injury starts on the medial side with either a rupture of the medial collateral ligaments or an avulsion of the medial malleolus.
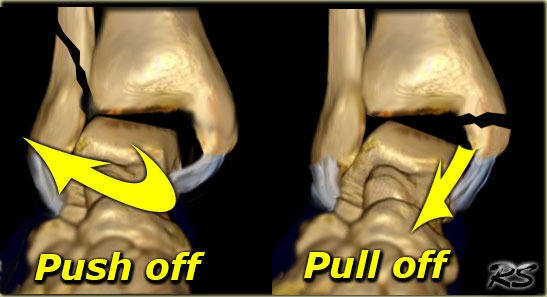
Pull-off or Push-off fractures
The shape of a fracture indicates which forces were involved.
An oblique or vertically oriented fracture indicates 'push-off'.
A transverse or horizontal fracture is the result of a 'pull-off' or avulsion.
On the left image the lateral malleolus is pushed off by exorotation of the talus.
On the right image the medial malleolus is pulled off by the medial collateral ligament due to pronation of the foot.
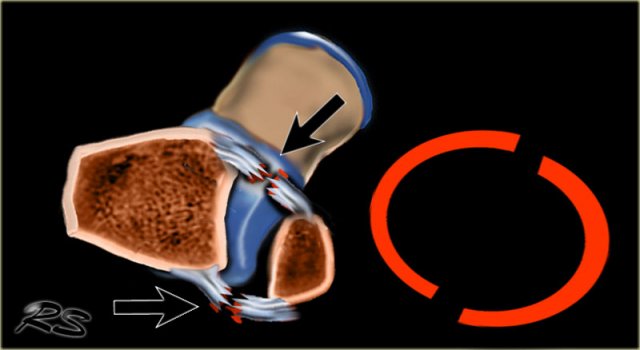
 Ring of stability in the coronal plane
Ring of stability in the coronal plane
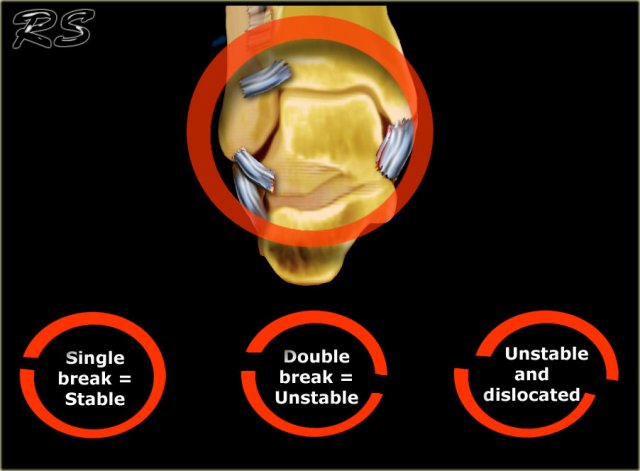
Stability
The ankle can be thought of as a ring in which bones as well as ligaments play an equally important role in the maintenance of joint stability.
If the ring is broken in one place the ring remains stable.
When it is broken in two places, the ring is unstable and may dislocate.
Now anyone can figure out, that an ankle is unstable when both the medial and the lateral malleoli are fractured.
It becomes more problematic when there is a combination of a fracture and a ligamentous rupture, because the ligamentous rupture is not detectable on the X-ray.
In some fractures there may even be a proximal fibular fracture - which is not visible on the ankle radiographs - in combination with ligamentous ruptures at the level of the ankle.
It is important to realize that in these cases the radiographs of the ankle may be normal, while there still is an unstable ankle injury.
 Ring of stability in the axial plane
Ring of stability in the axial plane
There is also an ring of stability in the axial plane.
When the anterior and posterior syndesmosis rupture or avulse, then the ankle joint is also unstable.
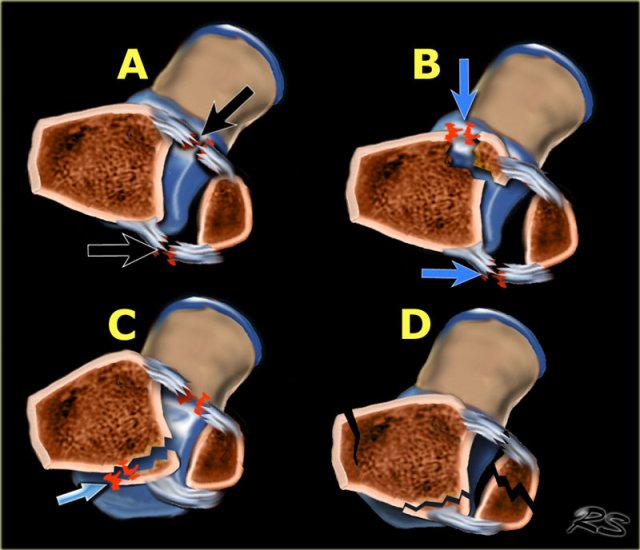
There are many combinations of avulsion fractures and ligamentous ruptures that can produce an unstable ring in the axial plane.
A
Anteriorly the anterior syndesmosis is usually one of the first structures to rupture. When the posterior syndesmosis also ruptures, then the ankle is unstable.
B
Less commonly the anterior syndesmosis avulses from the tibial attachment - Tillaux fracture.
C
On the posterior side frequently the posterior malleolus avulses. Sometimes these fractures are difficult to detect, as we will discuss in a moment.
D
After the injury the bones frequently align again, which makes it difficult to detect.
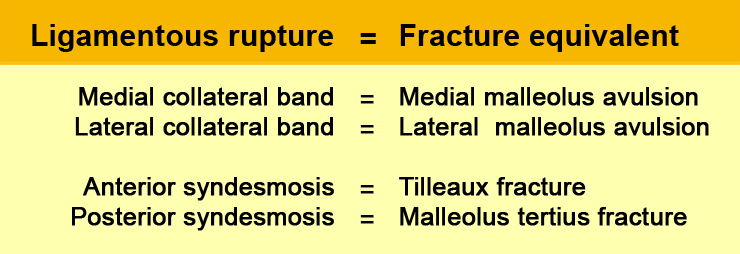
Stability (2)
It is important to realize, that for the stability of the ankle it doesn't matter whether there is a rupture of a ligament or an avulsion at the insertion.
Almost every ligamentous rupture has a fracture equivalent.

Stability (3)
On the left image a Weber A or SA-fracture.
This ankle is stable because there is only an avulsion fracture of the lateral malleolus below the level of the syndesmosis.
The ring is broken in only one place.
On the right image there is an unstable fracture.
The ring of the ankle is broken in two places.
There is a lateral fracture and on the medial side there is a rupture of the collateral ligament allowing the talus to dislocate laterally.
Stability (4)
The medial clear space should not exceed 4 mm and is usually equal to the distance between the tibial plafond and the talus.
Widening of the medial joint space up to 6 mm or more requires disruption of the medial collateral ligament.
Stability (5)
The lateral clear space is measured from the medial border of the fibula to the lateral border of the posterior tibia 1cm above the tibial plafond.
It is less well defined because its width varies with positioning.
Evident widening of the lateral clear space indicates syndesmotic rupture.
Some state that a width of 5.5 mm is abnormal.
It is very important to realize that a normal lateral or medial clear space does not exclude ligamentous rupture.
It simply means that there is no dislocation, but there can still be instability.
The case on the left shows a Weber B fracture.
On these images the ankle fork is normal.
Both the medial and lateral clear spaces are prominent, but within normal limits.
We can conclude that there is no dislocation, but we do not know if there is rupture of the medial collateral ligaments or of the syndesmosis.
Continue with the images post surgery.
Following osteosynthesis there is obvious widening of the medial and lateral clear spaces (image on the far left).
This indicates that there is a syndesmotic rupture and medial collateral ligament rupture.
The ring is still broken in two places.
The ankle joint is unstable and dislocated.
Resurgery was necessary with placement of a syndesmotic screw to stabilize the ankle joint.
Stability (6)
On the left another case. There is a Weber B fracture.
Both the medial and lateral clear spaces are widened, indicating instability.
The talus is displaced laterally.
Patient was scheduled for osteosynthesis of the fibular fracture and placement of a syndesmotic screw if necessary.
After osteosynthesis of the fibula, the ankle was tested in the operating room and found to be stable.
There was no indication for a syndesmotic screw.
It was concluded that the syndesmosis was only partially ruptured, as is usually the case in Weber B fractures.
The ring was broken in two places and after repairing one of them, the ring was stable.
Ottawa Ankle Rules

These rules are used to determine the need for radiographs in patients with an ankle injury.
Ankle X-ray series are only required in case of:
Pain in the malleolar zone and any one of the following:
- Bone tenderness along the distal 6 cm of the posterior edge of the fibula or tip of the lateral malleolus.
- Bone tenderness along the distal 6 cm of the posterior edge of the tibia or tip of the medial malleolus.
- Inability to bear weight for 4 steps both immediately and in the emergency department.
Radiography
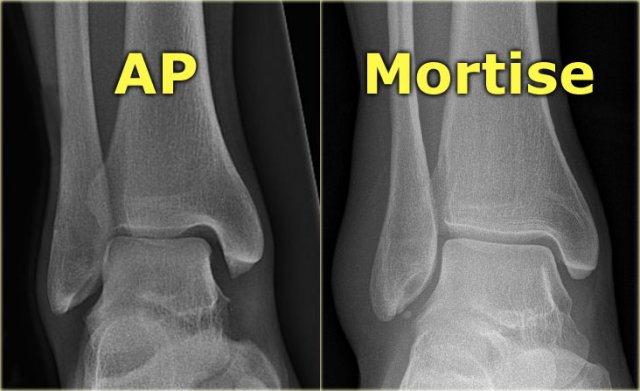
Mortise view
A basic radiographic examination of the injured ankle consists of an AP-view, a Mortise-view and a lateral view.
The Mortise-view is an AP-view taken with a 15-25? endorotation of the foot.
The technologist turns the foot inwards until the lateral malleolus is at the same height as the medial malleolus.
This view visualizes both the lateral and medial joint spaces.
On a true AP-view the talus overlaps a portion of the lateral malleolus, obscuring the lateral aspect of the ankle joint.
 The distal fibula should project on the posterior part of the distal tibia
The distal fibula should project on the posterior part of the distal tibia
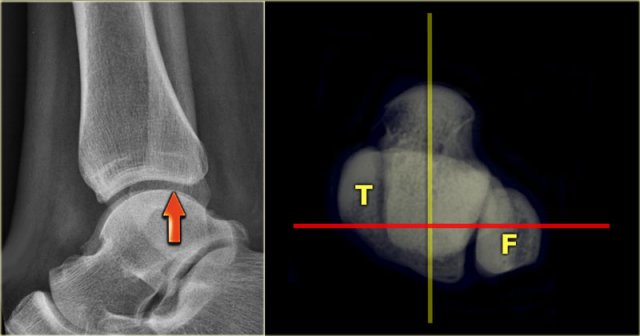
Lateral view
Many think that for a good lateral view the distal fibula should be in the center of the distal tibia.
However, since the fibula is positioned more dorsally, the fibula should project over the posterior part of the distal tibia (arrow).
 Malpositioning of the lateral view
Malpositioning of the lateral view
Malpositioning of the Lateral view
Malpositioning of the lateral view is the most common mistake in radiography of the injured ankle.
Because the patient is in pain, the technologist is afraid to let the patient turn the ankle fully lateral.
This is one of the reasons why we miss so many fractures of the posterior malleolus.
The CT demonstrates a large tertius fracture.
On the lateral view and also on the AP- and Mortise views, which will be shown in the paragraph on tertius fractures, this fracture was not visible.
The explanation is that on the lateral radiograph the fibula projects in the middle of the tibia.
The x-ray beam is not parallel to the fracture line.
Since the fracture line of a tertius fracture always has this orientation, we must insist on a true lateral view.
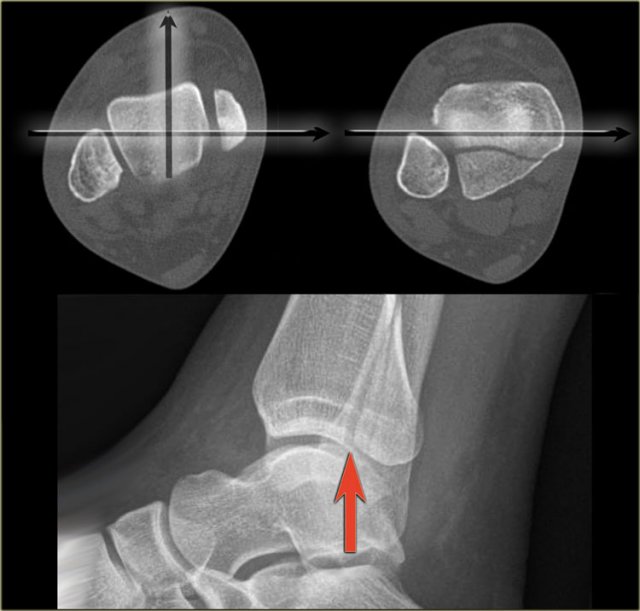 Good positioning of the lateral view - Tertius fracture
Good positioning of the lateral view - Tertius fracture
On a well positioned lateral view the tertius fracture is obvious (red arrow).
This was the only fracture that was seen on the x-rays of the ankle and this patient turned out to have an unstable Weber-C fracture and went for surgery.

The x-ray beam has to be centered on the malleoli.
Notice the exorotation of the foot for a proper lateral view.
Videos of severe ankle injuries
The forces in ankle injuries can be enormous.
As was discussed in Ankle fractures 1 the injuries usually take place in a logical sequence.
Start the video on the left by clicking on the image.
Notice that at first the foot is in supination with maximal forces on the lateral side.
Subsequently the foot adducts.
The result is an SA or Weber A fracture.
We can assume that this is a Lauge Hansen Supination Adduction injury stage 2.
Start the video on the left by clicking on the image.
Notice that at first the foot is in pronation, with maximum forces on the medial side.
Subsequently the foot exorotates.
The result is a PER - pronation exorotation injury or Weber C fracture.

Charity
All the profits of the Radiology Assistant go to Medical Action Myanmar which is run by Dr. Nini Tun and Dr. Frank Smithuis sr, who is a professor at Oxford university and happens to be the brother of Robin Smithuis.
Click here or on the image below to watch the video of Medical Action Myanmar and if you like the Radiology Assistant, please support Medical Action Myanmar with a small gift.