Ankle fractures - Weber and Lauge-Hansen Classification
Robin Smithuis
Radiology Department of the Alrijne Hospital, Leiderdorp, the Netherlands
Publicationdate
Classification of ankle fractures is important in order to estimate the extent of the injury and the stability of the joint.
The Weber classification focuses on the integrity of the fibula and the syndesmosis, which holds the ankle mortise together.
The Lauge-Hansen system focuses on the trauma mechanism.
Adding the stages of Lauge-Hansen to the Weber system will help you to predict ligamentous injury and instability.
This article will help you to correctly stage ankle injuries and to detect fractures, that are not obvious at first sight.
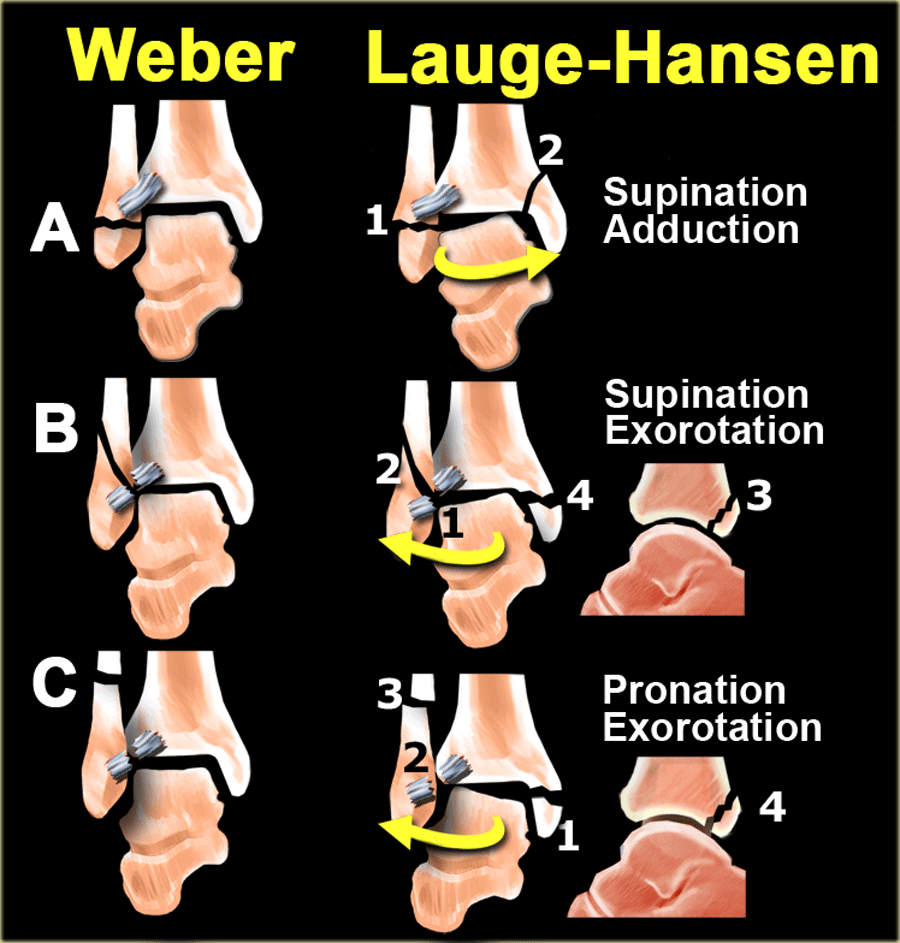
Short overview
Basically there are three main types of ankle fractures.
Weber classified them as:
- type A - infrasyndesmotic
- type B - transsyndesmotic
- type C - suprasyndesmotic
These fractures are identical to the fractures described by Lauge-Hansen as supination-adduction, supination-exorotation and pronation-exorotation.
We will first give a short overview of these fractures and then discuss them in more detail.
Once you understand the trauma mechanism as described by Lauge-Hansen and the sequence of events that take place in stages, then you know where to look for fractures and ligamentous injuries.
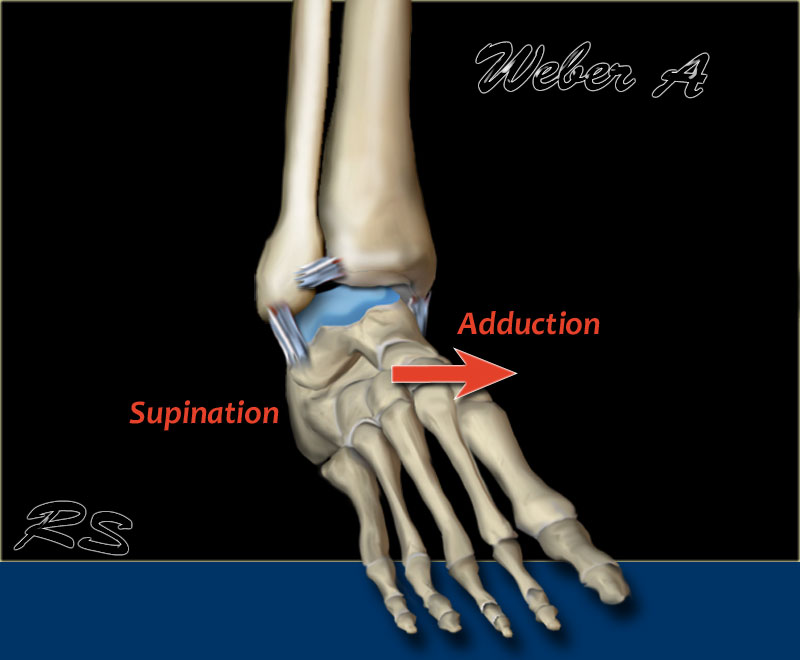
Weber A
Occurs below the syndesmosis, which is intact.
According to Lauge-Hansen, it is the result of an adduction force on the supinated foot.
- Stage 1 - Tension on the lateral collateral ligaments results in rupture of the ligaments
or avulsion of the lateral malleolus below the syndesmosis. - Stage 2 - Oblique fracture of the medial malleolus.
Scroll through the images.
Notice that the fibular fracture is transverse, because it is an avulsion or pull-off fracture.
The tibial fracture is vertical or oblique, because it is a push-off fracture.
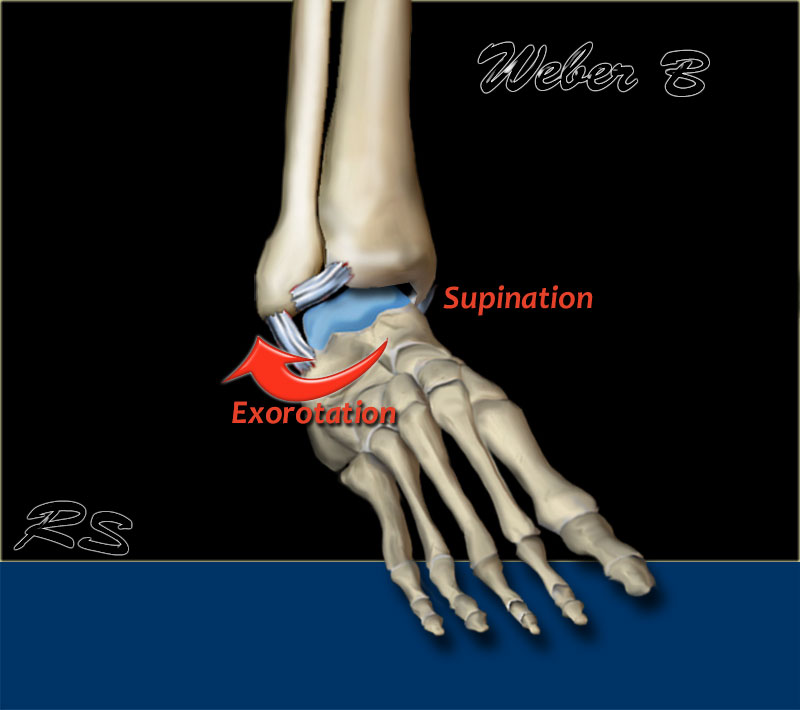
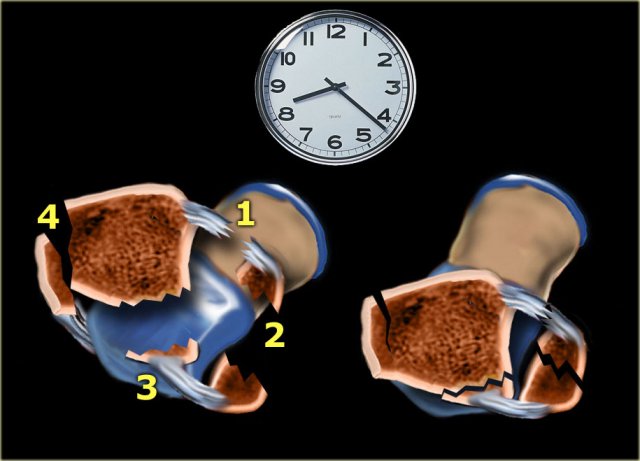
Weber B
This is a transsyndesmotic fracture with usually partial - and less commonly, total - rupture of the syndesmosis.
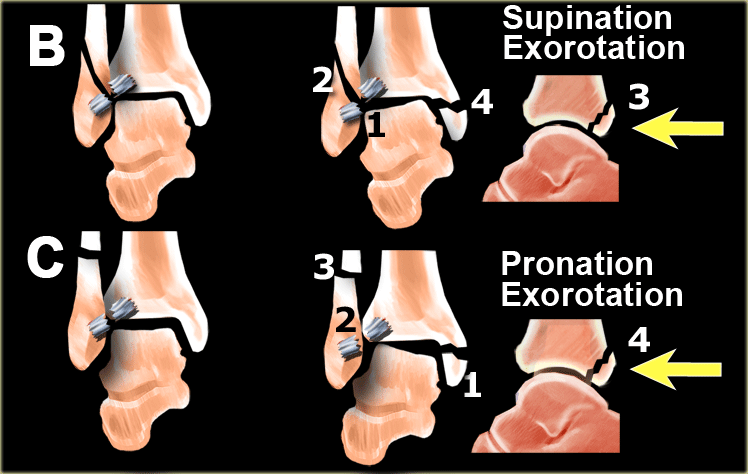
According to Lauge-Hansen, it is the result of an exorotation force on the supinated foot.
- Stage 1 - Rupture of the anterior syndesmosis
- Stage 2 - Oblique fracture of the fibula (this is the true Weber B fracture)
- Stage 3 - Rupture of the posterior syndesmosis
or - fracture of the posterior malleolus - Stage 4 - Avulsion of the medial malleolus
or - rupture of the medial collateral bands
Scroll through the images.
Notice the oblique or vertical orientation of the push-off fibular fracture.
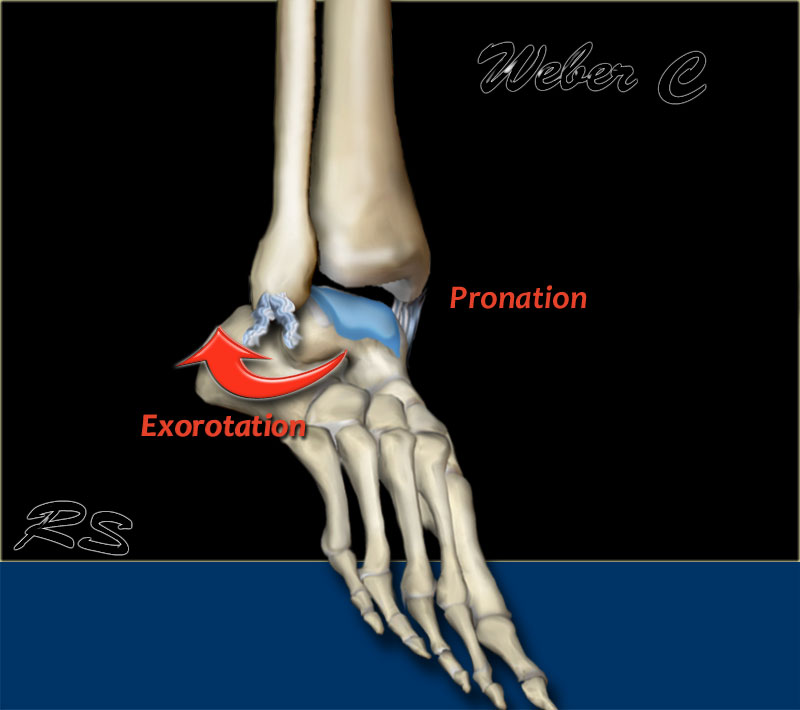
Weber C
This is a fracture above the level of the syndesmosis. Usually there is a total rupture of the syndesmosis with instability of the ankle.
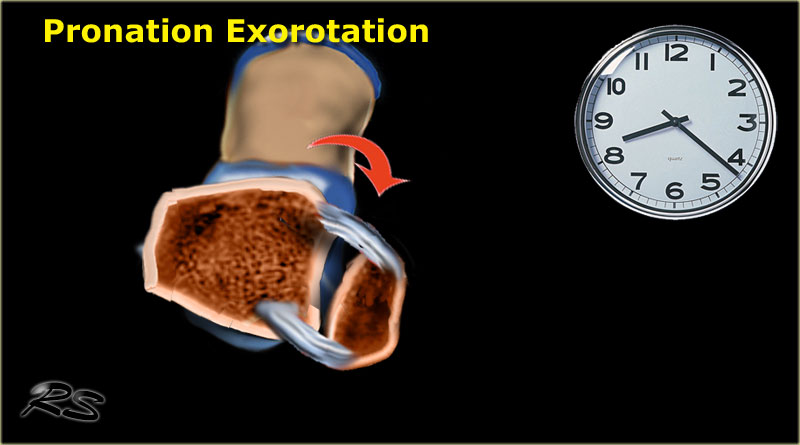
According to Lauge-Hansen, it is the result of an exorotation force on the pronated foot.
- Stage 1 - Avulsion of the medial malleolus
or - ligamentous rupture - Stage 2 - Rupture of the anterior syndesmosis
- Stage 3 - Fibula fracture above the level of the syndesmosis (this is the true Weber C fracture)
- Stage 4 - Avulsion of the posterior malleolus
or - rupture of the posterior syndesmosis
Scroll through the images
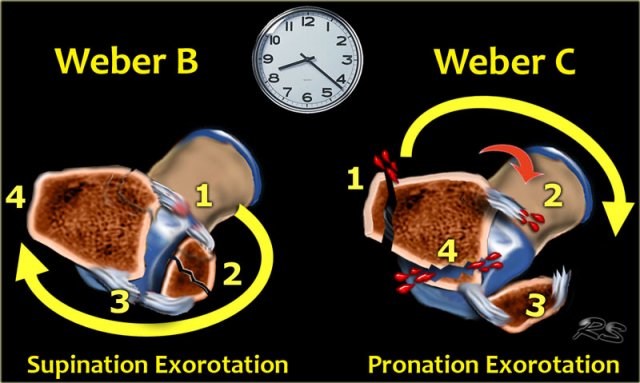
Exorotation injury
Weber A fractures are usually not a problem.
Weber B and C are more difficult and it is essential to understand the sequence of events in these injuries, which are both exorotation injuries.
This implies that 75-80% of ankle injuries are exorotation injuries.
Weber B starts anterolaterally and the sequence is:
- Anterior syndesmosis
- Fibula
- Posterior syndesmosis
- Medial malleolus
Weber C starts medially and the sequence is:
- Medial malleolus
- Anterior syndesmosis
- Fibula
- Posterior syndesmosis
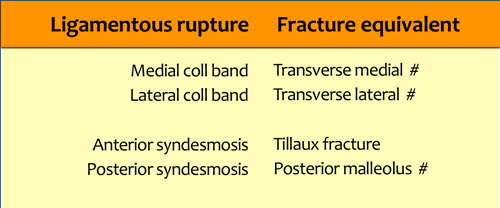
Ligamentous rupture or Avulsion
Another important thing to remember is, that a ligament can rupture or cause an avulsion fracture at the insertion.
Every ligamentous rupture has it's avulsion fracture counterpart.
Weber and Lauge-Hansen summary
-
Weber A = Infrasyndesmotic
- Avulsion of the lateral malleolus
- Oblique fracture of the medial malleolus (uncommon)
-
Weber B = Transsyndesmotic
- Rupture of the anterior syndesmosis
- Oblique fracture of the fibula
- Rupture of the posterior syndesmosis
or - fracture of the posterior malleolus - Avulsion of the medial malleolus -
or - rupture of the medial bands
-
Weber C = Suprasyndesmotic
- Avulsion of the medial malleolus
or - ligamentous rupture - Rupture of the anterior syndesmosis
- Fibula fracture above the level of the syndesmosis
- Avulsion of the posterior malleolus
or - rupture of the posterior syndesmosis
- Avulsion of the medial malleolus
Instability is seen in:
- Weber A stage 2
- Weber B stage 3 -4
- Weber C stage 3-4
Weber and Lauge-Hansen combined
In daily practice most use the Weber system, which is easy to memorize, while the Lauge-Hansen seems rather difficult at first glance.
Combining the simplicity of Weber with the explanation of the trauma mechanism given by Lauge-Hansen has the advantage that you still use a simple system, but now you really know what is going on.
For instance if you see a fracture that is a stage 2 in the Lauge-Hansen system, then you know that there also is a stage 1 injury and you will study the radiographs with a high suspicion for signs of stage 3 and 4.
This can best be demonstrated by giving an example.
 Unstable ankle fracture
Unstable ankle fracture
- First impression
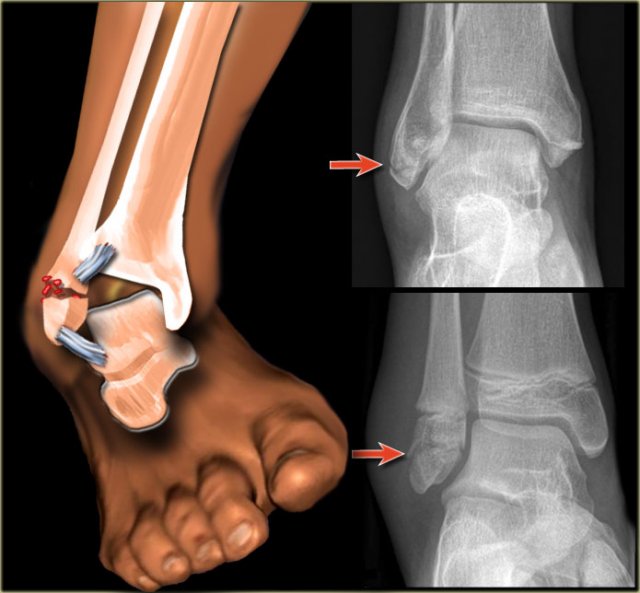
The radiographs show a fracture of the posterior malleolus.
If you would just report this as - a fracture of the posterior malleolus - you would miss the point.
This is probably an unstable ankle fracture.
A posterior malleolus fracture as an isolated finding is very uncommon.
- Looking at the classification system
When we look at the scheme we will notice that a fracture of the posterior malleolus in most cases is part of a Weber B or a Weber C fracture.
A tertius fracture is either Weber B stage 3
or - due to Weber C stage 4 (arrows).
We have to re-examine the films to look for additional findings.
Since we now know where to look, it will be easier to detect additional findings.
 PE stage 1
PE stage 1
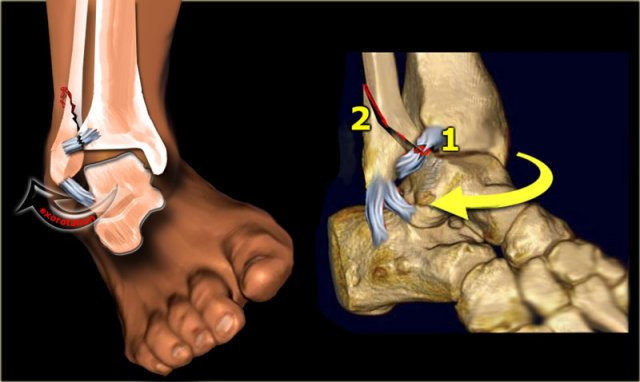
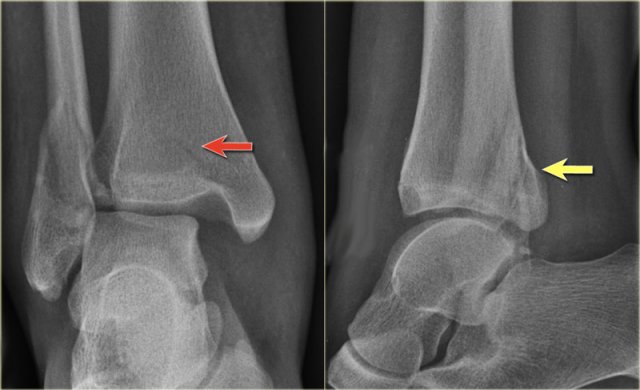
- Re-examination
On the ankle films there was no sign of an oblique fracture of the lateral malleolus, so we can exclude a Weber B fracture.
There is still the possibility of a Weber C fracture stage 4, i.e. medial rupture or avulsion, high fibular fracture and finally a posterior malleolus fracture.
At reexamination you notice the subtle avulsion of the medial malleolus (red arrow), which is stage 1.
Notice also the soft tissue swelling on the medial side (blue arrow)
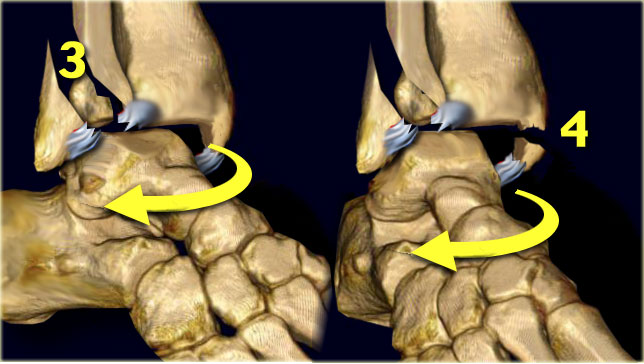
 PE stage 3
PE stage 3
Additional radiographs of the lower extremity were ordered and they demonstrate a high fibular fracture, i.e. Weber C stage 3 also known as a Maisonneuve fracture.
-
Final report
Weber C fracture stage 4.
This is un unstable ankle injury that needs surgical repair.
This example is an every day case.
The point that I want to make is, that when you understand the sequence of injuries to the ankle, then you know where to look for fractures and soft tissue swelling indicating ligamentous injury.
Weber A in detail
We will now discuss the Weber classification and add the stages of the Lauge-Hansen system.
Weber A is seen in 20-25% of all ankle fractures.
The diagnosis as well as the treatment is usually no problem.
According to Lauge-Hansen the fracture results from an adduction force on the supinated foot.
The lateral side is under extreme tension with stretch on the ligaments which results in an avulsion fracture.
Almost always the avulsion is seen as a horizontal fracture.
This is called a pull off type of fracture in contrast to a push off type, which is seen as an oblique or vertical fracture.
 Weber-A stage I
Weber-A stage I
Stage 1
The images show the usual Weber type A fractures.
These are all stage-1 fractures.
Stage-2 is extremely uncommon.
Notice the horizontal orientation of the fracture lines.
These are pull off type fractures as a result of avulsion.
 Weber A - stage 2
Weber A - stage 2
Stage 2
Stage 2 is uncommon and easy to detect.
More adduction force results in the medial malleolus being pushed off in a vertical or oblique way.
Stage 2 is unstable because the ring of the ankle is broken in two places.
Notice the horizontal orientation of the lateral malleolus fracture and the vertical orientation of the fracture of the medial malleolus.
Enormous forces must have pushed off the medial malleolus.
Weber B in detail
 Stage 1: Rupture of anterior tibiofibular ligament - or avulsion fracture (Tilleaux)
Stage 1: Rupture of anterior tibiofibular ligament - or avulsion fracture (Tilleaux)
Stage 1-2
Weber B is the most common type of ankle fracture and occurs in about 60 %.
According to Lauge-Hansen the fracture results from an exorotation force on the supinated foot.
Stage 1 is usually not visible on x-rays.
What we normally see is a stage 2 oblique fracture through the syndesmosis and we have to assume that there is also a rupture of the anterior tibiofibular ligament, which is stage 1.
According to Lauge Hansen the first injury is on the lateral side, which is under maximum tension.
In stage 2 the talus exorotates further and since the foot is in supination, the lateral malleolus is held tightly in place by the lateral collateral ligaments.
The lateral malleolus cannot move away without breaking.
As a result more rotation of the talus will fracture the fibula in an oblique or spiral fashion because the lateral malleolus is pushed off from anteromedially to posterolaterally.

The images show a Weber B fracture.
The oblique course of the fracture is typical for Weber B and results from the exorotation of the talus that pushes against the fixed lateral malleolus.
The malleolar fracture usually starts medially at the level of the talar dome, but can also start a few centimeters above this level.
 Weber B - stage 3 and 4
Weber B - stage 3 and 4
Stage 3-4
Stage 3 More posterior displacement of the lateral malleolus fragment by the talus results in tension on the posterior syndesmosis with rupture or avulsion of the posterior malleolus.
Stage 4 Further posterior movement of the talus will result in extreme tension on the medial side and the deltoid ligament will either rupture or pull off the medial malleolus in the transverse plane.
The sequences in a Weber B fracture or Lauge-Hansen supination exorotation injury take place in a clockwise manner:
- Rupture of the anterior tibiofibular ligament
- Oblique fracture of the distal fibula
- Avulsion of the posterior malleolus or rupture of the posterior tibiofibular ligament
- Avulsion of the medial malleolus or rupture of the medial collateral ligament
Immediately after the injury the injured parts may again align, which can make it difficult to detect the injuries.
 Weber B fracture
Weber B fracture
The radiographs show a typical Weber B fracture.
First study the images and then continue reading.
Do you see what stage this is?
This is a Weber B stage 4 injury.
Notice that all 4 stages are visible:
- Rupture of the anterior syndesmosis - seen as widening of the space between the distal tibia and fibula (lateral clear space).
- Oblique fibula fracture at the level of the syndesmosis - i.e. Weber B fracture.
- Tertius fracture - seen on AP view (red arrow) and on lateral view (yellow arrow).
- Rupture of the medial collateral ligaments - seen as widening of the space between the medial malleolus and the talus (medial clear space)

These images show another typical Weber B fracture stage 4.
There is an oblique fracture of the fibula.
There is an avulsion of the posterior malleolus and an avulsion of the medial malleolus.

Here another typical Weber B fracture stage 4.
First notice the oblique fibular fracture, which is best seen on the lateral view.
This is stage 2 and we have to assume, that the anterior syndesmosis is ruptured.
On the lateral view a small tertius fragment is seen indicating stage 3.
Now you start looking for stage 4 and you will notice the subtle lucency in the medial malleolus on the AP view (green arrow).
Knowing the stages of Lauge Hansen this must be a fracture.

Here a more subtle case.
At first impression there is a Weber B fracture stage 2.
Now we start looking for stage 3, which is a tertius fracture.
The small linear density on the AP-view is enough to diagnose a tertius fracture.
The soft tissue swelling on the medial side is probably a rupture of the medial collateral band , i.e. stage 4.
Weber C in detail
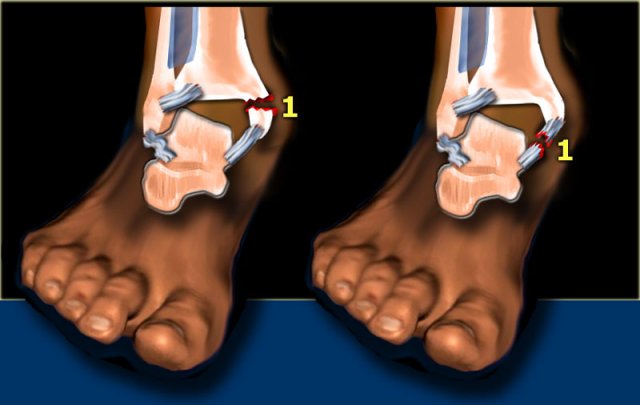
Stage 1
Weber C is seen in approximately 20% of ankle fractures.
It is the most difficult fracture to diagnose and the Lauge-Hansen system will help you to understand the fracture-mechanism, as this will be an enormous help.
According to Lauge-Hansen the fracture results from an exorotation force on the pronated foot.
Stage 1 The first injury will occur on the medial side, which is under maximum tension due to the pronation.
It will lead to rupture of the medial collateral ligament or avulsion of the medial malleolus.
Now the injury can stop and there will only be a rupture of the medial collateral ligaments or avulsion of the medial malleolus.
Lauge Hansen calls this PE stage 1.
We can not cathegorize this in the Weber classification, since there is no fibular fracture.
In many cases the injury progresses to a higher stage.
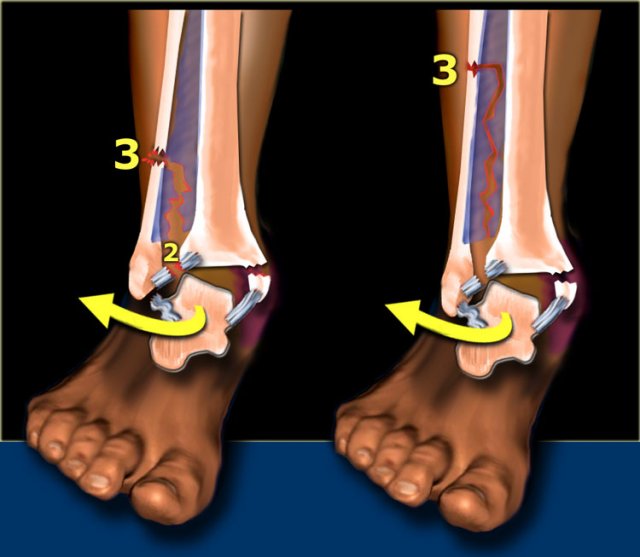
Stage 2-3
The talus rotates externally and moves laterally because it is free from its medial attachment.
Due to the pronation, the lateral ligaments are not under tension and the fibula can move away from the tibia.
This causes rupture of the anterior syndesmosis. This is stage 2.
Continuous force will twist the fibula and displace it distally, while proximally it is fixed to the tibia.
Finally the interosseus membrane will rupture up to the point where the fibular shaft fractures. This is stage 3.
This is always above the level of the syndesmosis.
In many cases it is visible on the radiographs of the ankle, but in some cases the fracture is located high and will only be visible on a radiograph of the lower leg.
This last type of fracture is also called Maisonneuve fracture.
Here we see the different stages in the axial plane.
- Medial avulsion fracture or rupture of the collateral band
- Rupture of the anterior syndesmosis
- Suprasyndesmotic rupture of the fibula due to rotation
- Posterior malleolus fracture or rupture of the posterior syndesmosis
Scroll through the images.
 Weber C fracture - stage 3
Weber C fracture - stage 3
The radiographs shows a Weber C fracture.
There is an avulsion fracture of the medial malleolus and a fibula fracture above the level of the syndesmosis.
According to Lauge-Hansen this is stage 3 pronation exorotation injury and so the anterior syndesmosis (stage 2) must also be ruptured.
We do not see a tertius fracture, which would indicate stage 4, but there may be a rupture of the posterior syndesmosis.
 Weber C fracture - at least stage 3
Weber C fracture - at least stage 3
Here an example of a Weber C fracture with a proximal fibula fracture.
Notice that on the radiograph of the ankle no fracture is seen.
You might misdiagnose this as only some soft tissue swelling.
In fact this is an unstable ankle fracture, since there also must be a rupture of the medial collateral ligament (stage 1) , so the ring is broken in two places leading to instability.
According to Lauge Hansen we are probably dealing with:
- Medial collateral band rupture
- Rupture of the anterior syndesmosis
- High fibula fracture
- and possibly a rupture of the posterior syndesmosis

Stage 4
Finally the posterior syndesmotic ligament ruptures, or there is an avulsion of the posterior malleolus, also known as posterior malleolus fracture (red arrow).
The medial clear space is only slightly widened, but based on the stages of Lauge Hansen there must be a collateral band rupture.
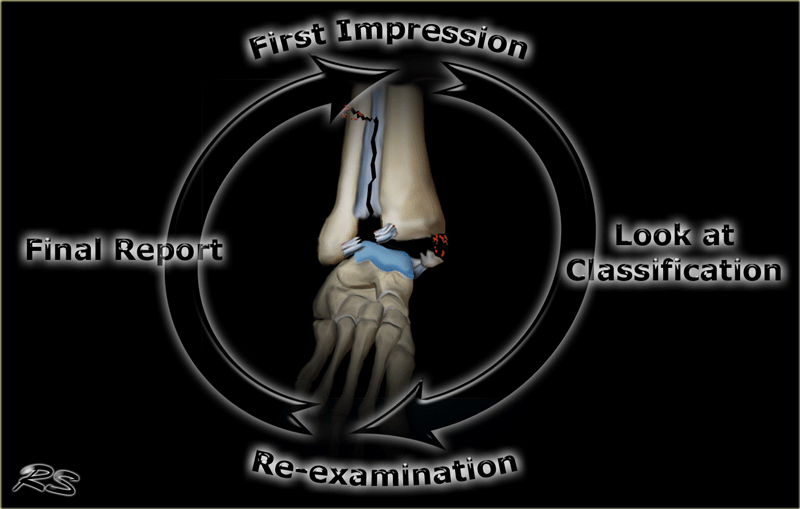
Interpretation and Reporting
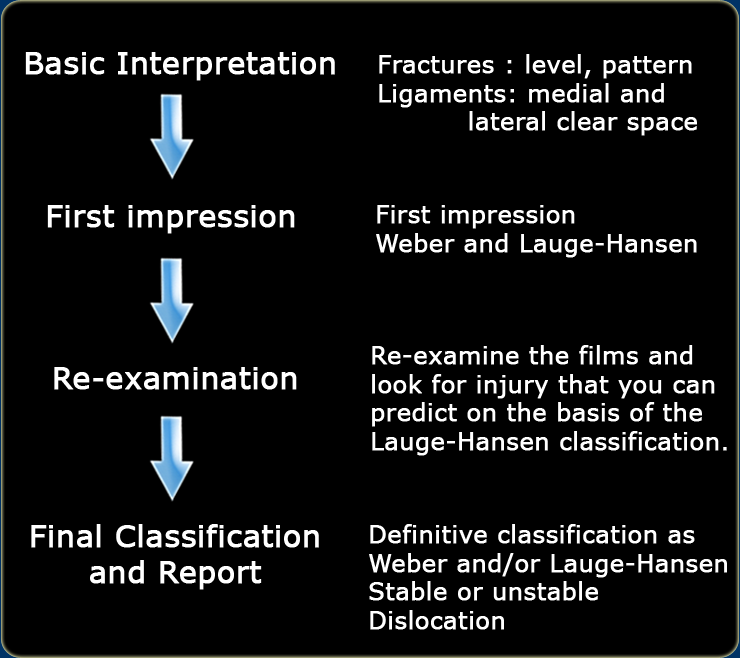
Start with a first impression and look for fractures and signs of ligamentous rupture.
This impression will direct you to both a Weber as well as a Lauge-Hansen classification.
The Lauge-Hansen classification will give you the fracture mechanism and the preliminary stage of the ankle injury.
Now re-examine the films to make sure that you do not overlook a higher grade ankle injury.
After this re-examination you can make a final report.
In the final report the fracture is described according to Weber and/or Lauge-Hansen.
Describe the number of malleoli involved and whether there are signs of instability or dislocation.
 Click to enlarge
Click to enlarge
Example 1
- Basic interpretation
There is a medial malleolar fracture.
You interprete this as an avulsion fracture. - Classification
Not possible to classify according to Weber, but according to Lauge Hansen a medial avulsion fracture indicates that the foot probably was in pronation at the moment of injury.
So this injury is probably a pronation exorotation injury (PER) stage 1 or higher.

- Re-examination
You re-examine the x-rays to look for stage 2 (rupture or avulsion of the anterior syndesmosis), stage 3 (high fibular fracture = Weber C) or even stage 4 (rupture or avulsion of posterior syndesmosis).
So at second look you notice a subtle widening of the lateral clear space on the original films, which could indicate but is definitely no proof of a syndesmotic rupture.
Although the patient is already in a cast you order additional films to look for a possible stage 3.
These films show a high fibular fracture and a subtle posterior malleolus avulsion. - Final report
Weber C fracture or a PER stage 4 according to Lauge-Hansen. This is an unstable fracture that needs surgical repair.
The ankle circle is interrupted at two places i.e. the medial malleolus and the syndesmosis.
A syndesmotic screw was inserted.

Example 2
- Basic interpretation
Transverse lateral malleolar fracture. -
Classification
Weber A and Supination Adduction stage 1. -
Re-examination
No sign of SA stage 2 (medial malleolar fracture) - Final report
Stable Weber A or SA stage 1 fracture.
Patient will be treated conservatively.

Example 3
- Basic interpretation
Dislocated bimalleolar fracture. Avulsion fracture of the medial malleolar.
The lateral malleolus is 'pushed off' from anterior to posterior. - Classification
The fracture starts at the level of the ankle joint and extends proximally, i.e. a Weber B fracture.
According to Lauge Hansen the oblique fibular fracture indicates Supination Exorotation injury stage 2 or higher. - Re-examination
Look for stage 3 (posterior syndesmotic rupture or avulsion of the posterior malleolus) and stage 4 (rupture of the deltoid ligament or medial malleolar avulsion).
Only now you notice the posterior malleolar fracture on the lateral view. - Final report
Trimalleolar fracture. Weber B. SER stage 4 (Lauge-Hansen).
This is an unstable fracture with dislocation that needs surgical repair.
The size of the posterior malleolar fragment is probably less than 25% of the articular AP-diameter and will need no separate repair.
Sometimes CT is needed to get a better impression of the size of the fracture fragment of the posterior malleolus.
 Click to enlarge
Click to enlarge
Example 4
- Basic interpretation
Fracture of the lateral malleolus starting anteriorly at the level of the joint extending proximally posteriorly. - Classification
The fracture is classified according to Weber as a type B fracture.
According to Lauge Hansen the oblique fibular fracture indicates that this is a Supination Exorotation injury stage 2 or higher. - Re-examination
Look for stage 3 and stage 4.
There are subtle findings which indicate a fracture of the posterior malleolus. Normally you probably would not have noticed these.
On the lateral view the posterior cortex of the tibia is interrupted indicating a fracture (blue arrow).
Even on the AP-view there are subtle findings that indicate a fracture (red arrows).
There is a widened medial clear space, which indicates a rupture of the medial collateral band, i.e. stage 4. - Final report
Weber B fracture. According to Lauge-Hansen this is a SER stage 4.
This is an unstable fracture with dislocation that needs surgical repair.

Charity
All the profits of the Radiology Assistant go to Medical Action Myanmar which is run by Dr. Nini Tun and Dr. Frank Smithuis sr, who is a professor at Oxford university and happens to be the brother of Robin Smithuis.
Click here or on the image below to watch the video of Medical Action Myanmar and if you like the Radiology Assistant, please support Medical Action Myanmar with a small gift.