Meniscus special cases
Robin Smithuis
Radiology department of the Rijnland hospital in Leiderdorp, the Netherlands
Publicationdate
In this article we will show some examples of special meniscal pathology in more detail.
For the basics of meniscal pathology we advise you first to read the article 'Knee Meniscus - Part 1'.
On most images you can click to get an enlarged view, but this does not work on the iPhone application.
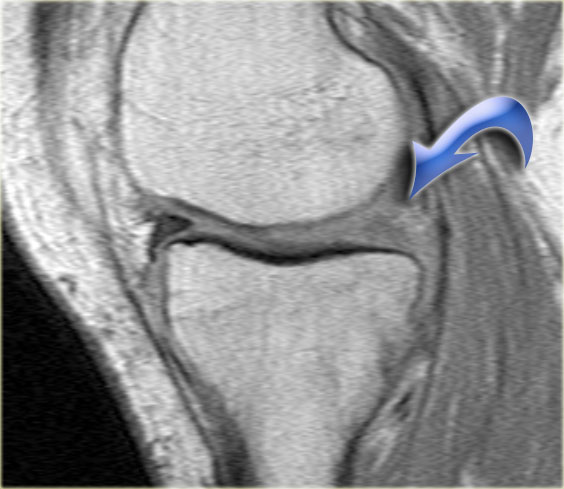
Flipped meniscus

Study the image on the left and try to determine what the problem is with this meniscus.
Then continue with the next consecutive images of the same patient.
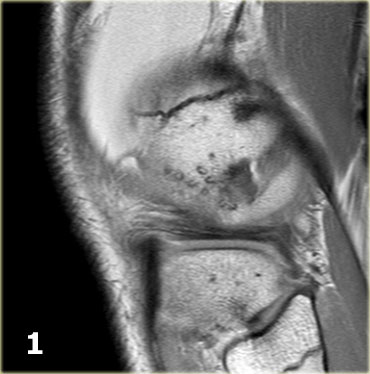
Scroll through the images.
Then continue reading..
As you already suspected by reading the title of this paragraph, this is a flipped meniscus.
A flipped meniscus is a special form of bucket-handle tear.
A flipped meniscus occurs when the ruptured fragment of the posterior horn is flipped anteriorly so the anterior horn of the meniscus appears to be enlarged.
- Body of lateral meniscus.
- Posterior horn is too small and anterior horn seems enlarged with an irregular contour.
- At first impression there is a longitudinal tear in the anterior horn, but actually the posterior part of this structure is the flipped part of the ruptured posterior horn.
The anterior structure is the anterior horn.
Also notice the focal bone marrow edema and the cartilage impression. - The anterior structure is the anterior horn.
- Some irregularity of the posterior part.
- Posterior part moves caudally.
- In the intercondylar fossa is the connection between the displaced fragment and the other part of the posterior horn.

On the left another flipped meniscus.
Now on the medial side.
Part of the anterior horn is flipped posteriorly.
Only a small part of the anterior horn is seen anteriorly.
Most flipped menisci occur on the lateral side.
The ACL prevents the meniscal fragment from completely migrating into the intercondylar notch.
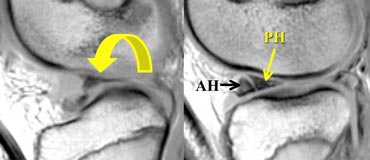
Illustration of the mechanism in a flipped meniscus.
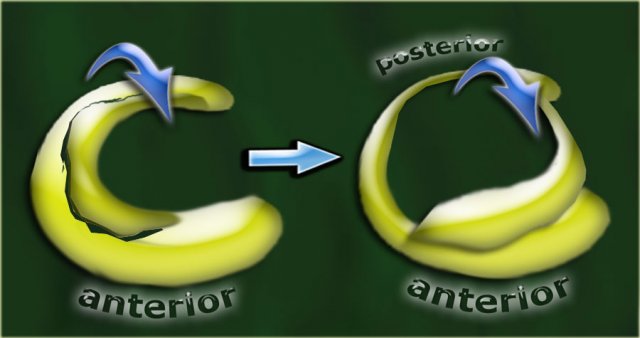
On a coronal image you will first see an enlarged bulky anterior horn.
Posteriorly a very small posterior horn will be seen.
See next case.
On the left another case of a flipped lateral meniscus.
Scroll through the images.
- Notice the very large anterior horn.
The medial part is the displaced posterior horn. - Medial part runs into the intercondylar fossa.
- The dislocated part is well seen as 'third structure'
in the intercondylar fossa. - Connection to the remnant of the posterior horn.
- Connection to the remnant of the posterior horn.
- Very small remnant of the posterior horn.

Same case sagittal images.
Notice how the ruptured part of the meniscus runs anteriorly through the intercondylar fossa (arrows)
- Normally only two structures run in the intercondylar fossa. Here we see the normal posterior cruciate ligament.
- Normal anterior cruciate ligament.
- Ruptured part of the posterior horn as 'third structure'
in the intercondylar fossa. - Ruptured part runs anteriorly.
- Ruptured part joins the anterior horn and simulates a longitudinal tear in the anterior horn.
Notice the small remnant of the posterior horn.
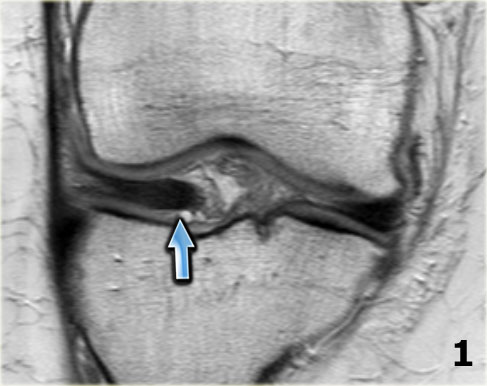
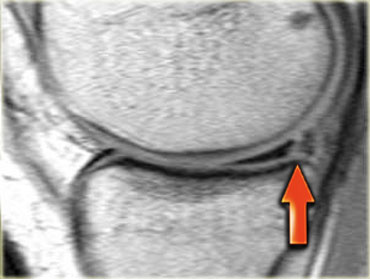
On the left sagittal PD-images of a flipped meniscus.
The whole posterior horn is flipped anteriorly resulting in an empty meniscus sign (arrow).
Bucket handle tear

First study the images on the left.
Then continue reading.
-
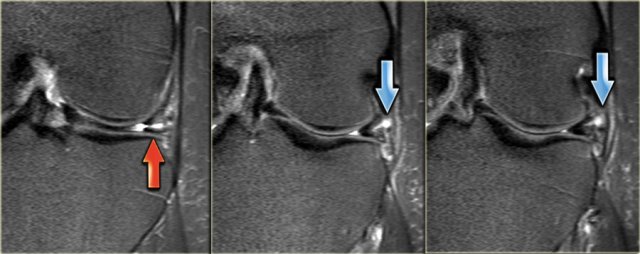
We start with a middle section of the examination.
Notice the small body of the lateral meniscus with an abnormal shape (blue arrow).
The missing inner part is seen just lateral to the anterior cruciate ligament (red arrow). - The medially displaced part of the torn meniscus, i.e. the bucket handle can be followed in a posterior direction in the intercondylar fossa.
- Continue.
- Here is the connection between the bucket handle and the posterior horn.
- Here an anterior slice demonstrating a meniscal cyst.
- Notice the horizontal high signal.
- Here we can appreciate the complexity of the meniscal tear with a longitudinal and horizontal component (arrows).
Bucket handle tears are displaced vertical longitudinal tears.
The displaced inner fragment resembles the handle of a bucket.
The remaining larger peripheral portion of the meniscus resembles the bucket.
These tears account for about 10% of all meniscal tears.
Double PCL sign

The double posterior cruciate ligament (PCL) sign is a low-signal-intensity band that is parallel and anteroinferior to the PCL on sagittal MR images.
It is a highly specific indicator of a bucket-handle meniscal tear (3).
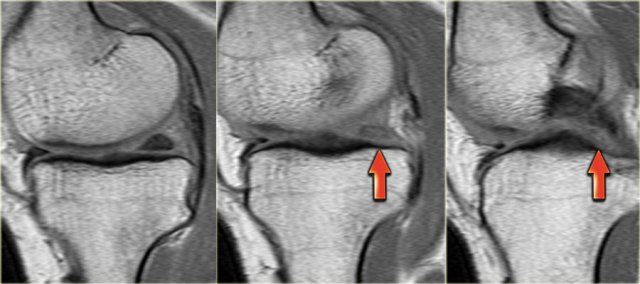
Meniscal root tear
First study the image on the left and try to recognize the meniscal tear.
These tears often go unnoticed.
Then continue with the next images.

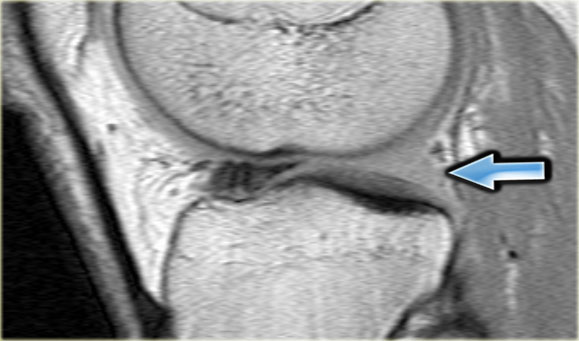
A radial tear is present at the posterior root junction of the medial meniscus which extends through the entire thickness of the meniscus with a cleft of fluid tracking through the defect (red arrows).

Meniscal root tears are often associated with extrusion of the meniscus beyond the margin of the tibial plateau.
More than 3 mm meniscus extrusion is often associated with tears involving the meniscal root (6).
In the case on the left there is a complete radial tear separating the posterior horn from its root (red arrows).
There is also minimal extrusion of the meniscus (image 1/6).
Here another medial meniscal root tear.
Notice that the posterior horn is not attached to the tibia.
Instead there is a gap (curved arrow).
You can easily overlook these tears and think that the posterior horn is normal.

This is another typical case of a medial meniscal root tear.
Notice that there is also a lateral discoid meniscus.
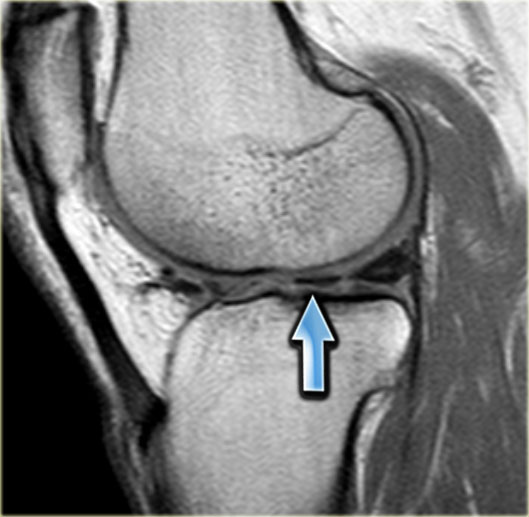
Empty meniscus sign
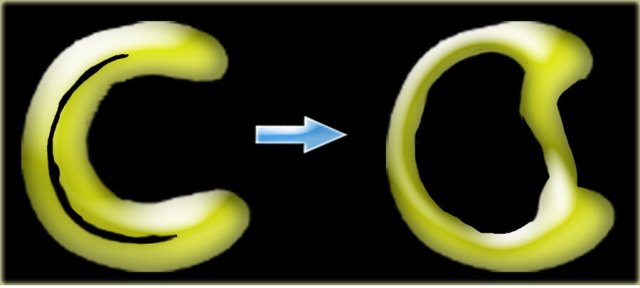
When there is a complete radial tear, the two meniscal fragments can be completely separated.
This can result in an empty meniscal space or empty meniscus sign (arrow).
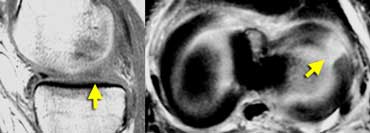 LEFT: Absent or empty meniscus on sagittal image. RIGHT: Axial image shows complete radial tear leading to a defect in the meniscus.
LEFT: Absent or empty meniscus on sagittal image. RIGHT: Axial image shows complete radial tear leading to a defect in the meniscus.
If you image a complete radial tear directly along the length of the tear you will see an absent or empty meniscus.
These complete radial tears open up and give the impression that there is a part missing.
However you will not find a displaced meniscal fragment.
It is simply separation of the meniscal parts.
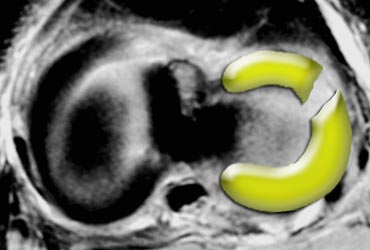
On the left an illustration of a complete radial tear, which can result in an empty meniscus sign.

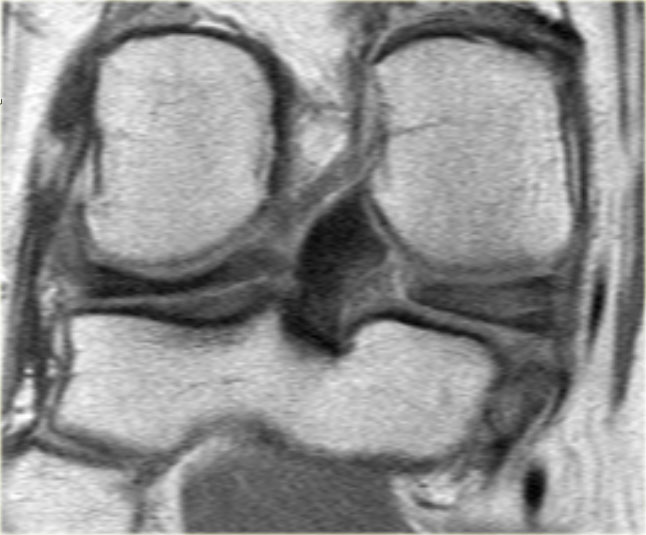
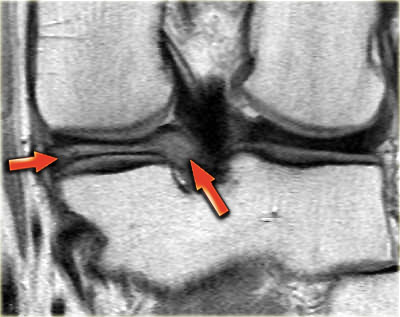
On the left coronal PD-images of a patient with a complete radial tear resulting in an empty meniscus sign.
- 1/7: Empty meniscus sign (horizontal red arrow).
- 2/7: Small remnant of body is seen.
- 3/7: Normal meniscal root attachment (blue arrow).
- 4/7: Normal posterior horn.
- 5/7: Anteriorly there is extrusion of the meniscus.
- 6/7: Extrusion.
- 7/7: Significant extrusion of more than 3 mm (red vertical arrow).
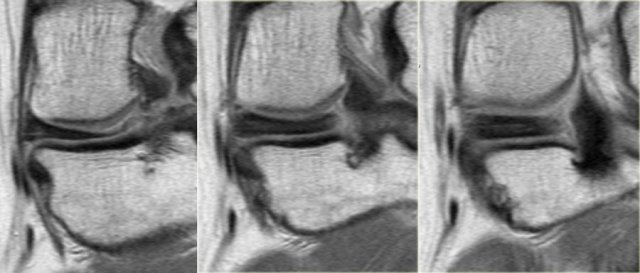
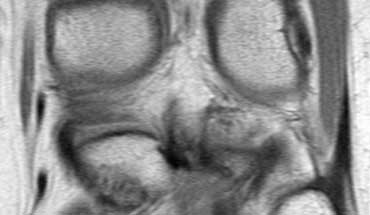
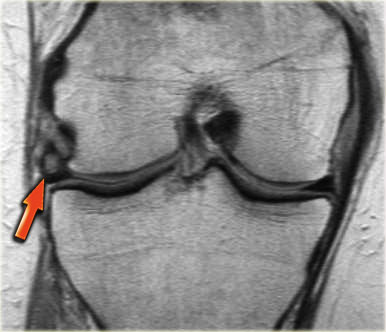
On the left consecutive coronal PD-images of a posterior horn of a meniscus that at first glance might give the impression that it is normal.
Continue with the sagittal images.
When you take a good look at the sagittal images, you will notice the empty meniscus sign, where normally the meniscal root attaches (red arrows).
This means that we are dealing with a meniscal root tear.
The meniscus posteriorly should come up over the tibial spine to insert near the posterior cruciate ligament.
Vacuum phenomenon
First scroll through the images on the left.
Try to figure out what is going on with this meniscus.
Then continue reading.
At first impression this looks like a tear within a discoid meniscus.
At closer look you will notice that the horizontal structure has a lower signal intensity than the meniscus and looks funny.
This is a normal variant caused by a vacuum phenomenon.
A vacuum phenomenon is caused by negative pressure within the joint due to the position of the patient, which results in the accumulation of nitrogengas.
Continue with the radiograph of the same patient.
Vacuum phenomenon on the lateral side.
Discoid Meniscus
First scroll through the images on the left.
Try to figure out what is going on with this meniscus.
Then continue reading.
The hypointense structure on the lateral side is a discoid meniscus (blue arrow).
The structure on the medial side is again a vacuum phenomenon.
On an adjacent slice this vacuum phenomenon is not seen any more.
Red zone meniscal tear
First scroll through the images on the left.
Try to figure out what is going on with this meniscus.
Then continue reading.
There is a longitudinal tear in the periphery of the meniscus (red arrow).
The outside one-third of the meniscus is called the 'red' zone, because it has a rich blood supply.
The location of a meniscal tear is of importance because tears in this vascular portion of the meniscus are more likely to heal spontaneously than tears in the avascular portion or white zone of the meniscus.
Meniscus within meniscus sign
Sometimes extensive triangular or wedge-shaped high signal intensity can be encountered that does not reach te surface of the meniscus.
This is sometimes referred to as meniscus within meniscus sign.
Since this meniscal abnormality does not reach the meniscal surface, it does not fullfill the criteria for a meniscal tear.
It was found that in half of these patients and symptoms warranting arthroscopic follow-up had meniscal tears (4).
On the left another meniscus with diffuse high signal in the meniscal body.
On other images (not shown) there was no evidence of a tear.
Notice severe extrusion of the meniscus beyond the margin of the tibia plateau.
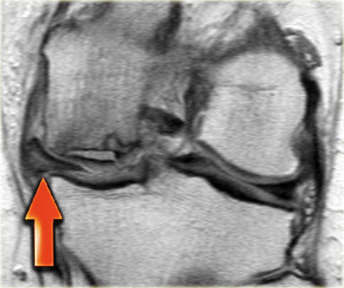
- Meniscus within meniscus sign and extrusion of middle part of meniscus (red arrow).
- Complete radial tear in the posterior horn.
Also notice the avascular necrosis. - Also notice the avascular necrosis.
- Extrusion of meniscus avascular necrosis.
Meniscal extrusion


Tears involving the meniscal root (central attachment) are also significantly related to the severity of meniscal extrusion, seen in 3% with minor extrusion and 42% with major extrusion.
With meniscus extrusion, the meniscus is unable to resist hoop stresses and cannot shield the adjacent articular cartilage from excessive axial load.
Over time, this can lead to symptomatic knee osteoarthritis.
Tears of the posterior meniscal root can be easily missed because of inconsistent clinical symptoms and can be overlooked without thorough arthroscopic examination.
Detection of meniscal extrusion is important not only because it is associated with underlying tear but also because meniscal extrusion itself is thought to be related to development of osteoarthritis.
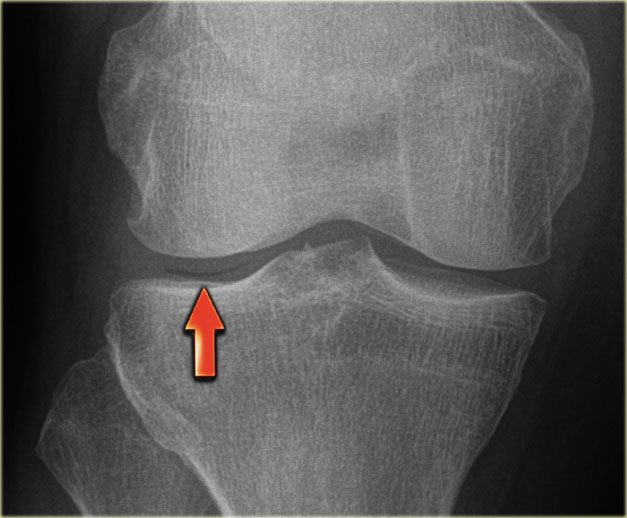
Segond fracture and meniscal tear
A Segond fracture is an avulsion of the lateral capsular ligament.
The mechanism of injury is internal rotation and varus stress.
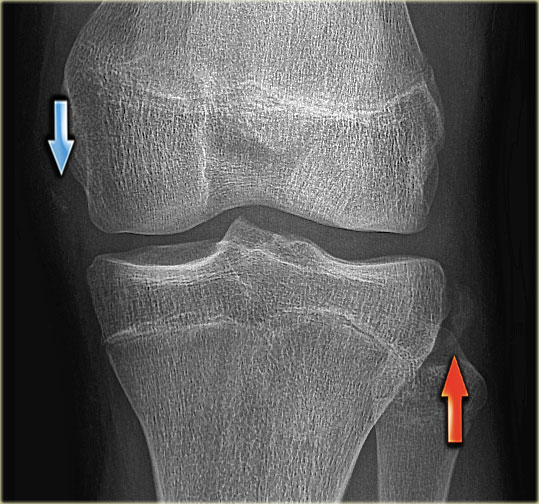
On a radiograph it manifests as an elliptic bony fragment off the lateral proximal tibia (figure).
A Segond fracture has a high association with a tear of the anterior cruciate ligament (75-100%) and injuries of the medial and lateral menisci (66-70%).
On the radiograph you could easily miss the Segond fracture (red arrow).
Notice that there is also an avulsion of the medial collateral ligament.
Continue with the MR-images.
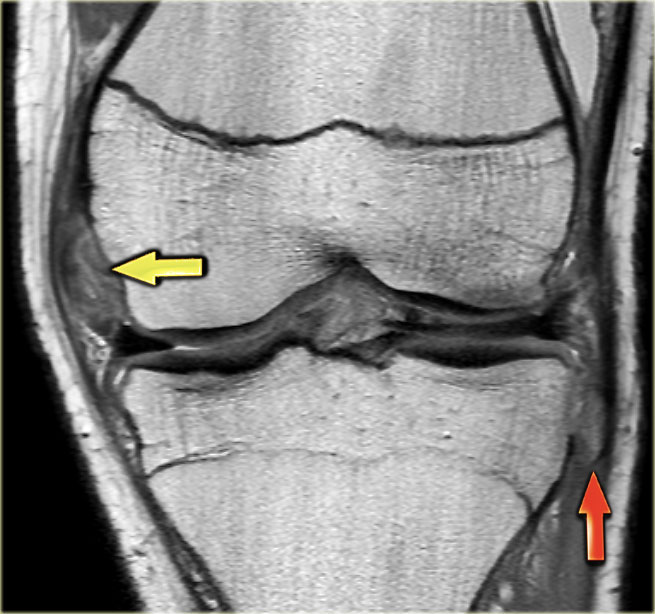
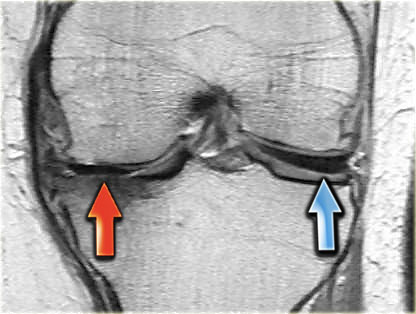
On the left three consecutive coronal PD-images:
-
Tear of deep medial collateral band (yellow arrow).
Avulsion of bone fragment of lateral proximal tibia, i.e. Segond fracture (red arrow). -
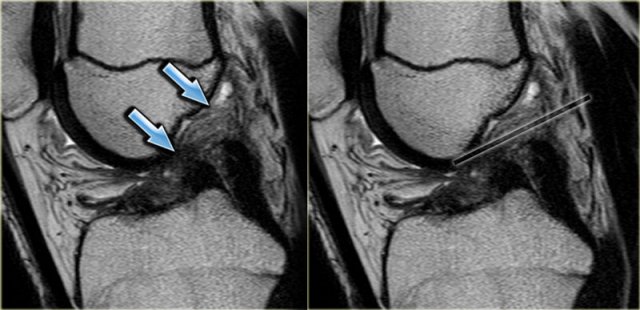
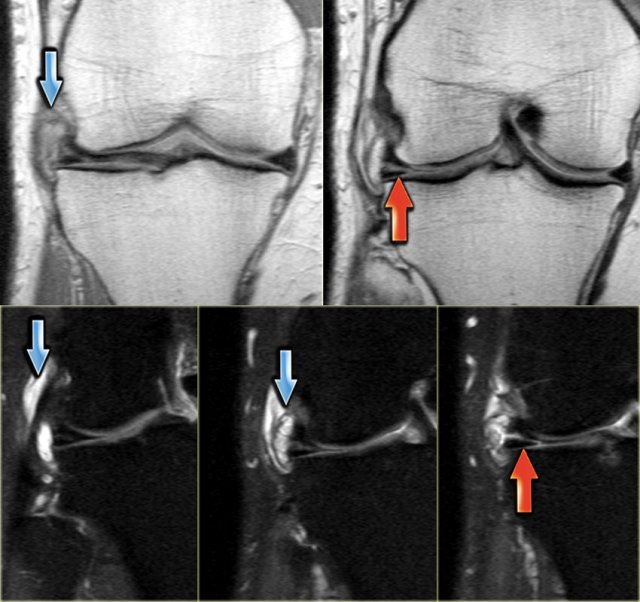
Notice displaced inner fragment of the meniscus.
This indicates that there is also a bucket handle tear. -
Besides the bucket handle tear (inner blue arrow), there is also a barely visible horizontal tear in the peripheral part of the meniscus (outer blue arrow).
The horizontal tear was better appreciated on other images (not shown).
Continue with the sagittal images.
A Segond fracture is almost pathognomonic for an anterior cruciate ligament tear, which was also demonstrated in this patient.

On the left an AP-view of another patient.
In association with a Segond fracture (red arrow), there is also an avulsion fracture of the anterior cruciate ligament (blue arrow).
Meniscal cyst
A meniscal cyst results from extrusion of synovial fluid through a peripherally extended horizontal meniscal tear.
Medial meniscal cysts are most commonly located adjacent to the posterior horn and lateral meniscal cysts are most commonly located adjacent to the anterior horn or body.
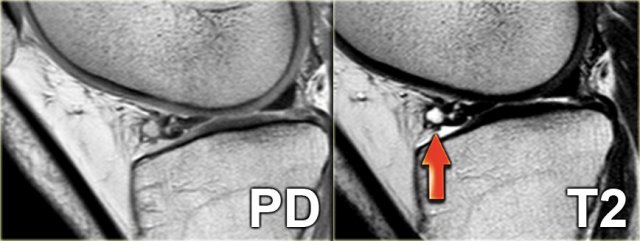
On the left a PD- and a T2-weighted image demonstrating a lateral meniscal cyst are adjacent to the anterior horn as a result of a complex tear.
On the left three consecutive images of a small meniscal cyst (blue arrow) as a result of a horizontal tear (red arrow).
On the left coronal PD-images without fatsat and with fatsat.
A large meniscal cyst is seen in relation to a horizontal tear (red arrow).