Shoulder instability - MRI
Robin Smithuis and Henk Jan van der Woude
Radiology department of the Rijnland hospital, Leiden and the Onze Lieve Vrouwe Gasthuis, Amsterdam, the Netherlands
Publicationdate
A Bankart lesion is an injury of the anterior glenoid labrum due to anterior shoulder dislocation.
These labral tears make the shoulder unstable and susceptible to repeated dislocations.
In this article we will focus on:
- Shouder dislocations
- Bankart tears and variants
Introduction
 Clockwise approach. Click on image to enlarge
Clockwise approach. Click on image to enlarge
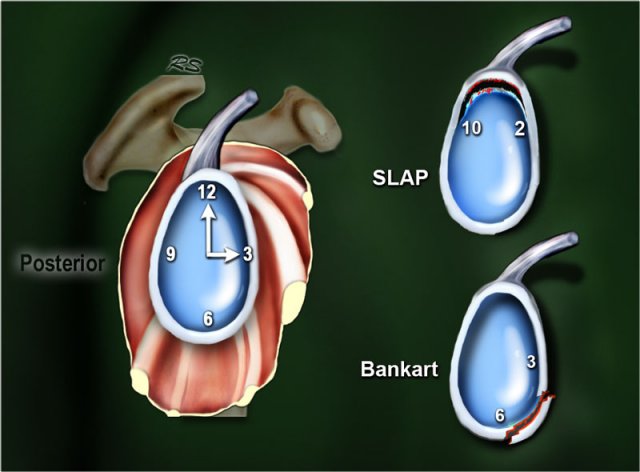
Clockwise approach to labral pathology
A Clockwise approach to the labrum is the easiest way to diagnose labral tears and to differentiate them from normal labral variants.
There are two types of labral tears: SLAP tears and Bankart lesions.
SLAP is an acronym that stands for 'Superior Labral tear from Anterior to Posterior'.
SLAP tears start at the 12 o'clock position where the biceps anchor is located, which tears the labrum off the glenoid.
SLAP tears typically extend from the 10 to the 2 o'clock position, but can extend more posteriorly or anteriorly and even extend into the biceps tendon.
Bankart lesions are typically located in the 3-6 o'clock position because that's where the humeral head dislocates.

There are many labral variants that may simulate a labral tear.
They also have a typical location.
They are not in the 3-6 o'clock position, which makes it easy to differentiate them from a Bankart tear.
A Bankart tear can extend to the 1-3 o'clock position, but then there should also be a tear in the 3-6 o'clock position.
Labral variants however may mimick a SLAP tear.
Dislocation

The shoulder is a very mobile and therefore unstable joint.
It is the most dislocated joint in the body.
The shoulder most commonly dislocates in an anterior and inferior direction, as superior motion is restricted by the acromion, coracoid process, and rotator cuff.
Posterior motion is limited by the posterior rim of the glenoid, which is typically in an anteverted position.
Posterior dislocations are uncommon and seen due to seizures, electric shock or in patients with dysplasia of the glenoid.

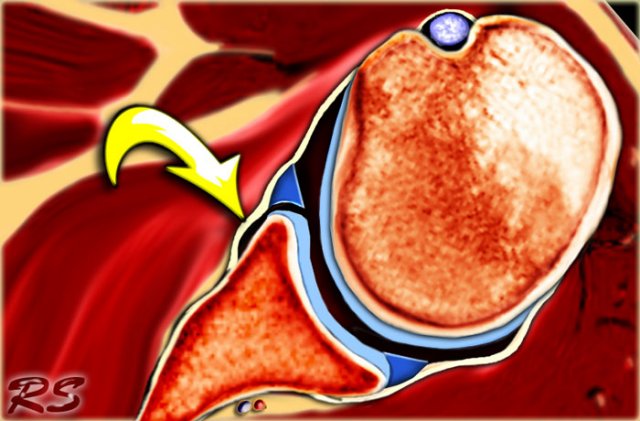
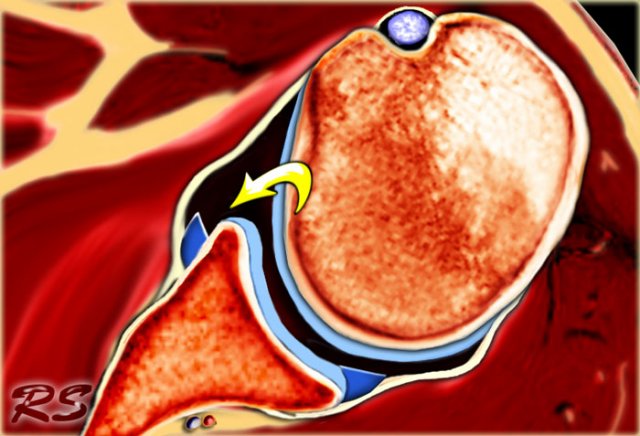
Anterior dislocation
The shoulder most commonly dislocates in an anterior and inferior direction, as superior motion is restricted by the acromion, coracoid process, and rotator cuff (Figure).
Posterior motion is limited by the posterior rim of the glenoid, which is typically in an anteverted position (red arrow).

The dislocation of the humeral head to antero-inferior causes damage to the antero-inferior rim of the glenoid in the 3 - 6 o'clock position (marked in red).
Especially in younger patients this results in a Bankart fracture or a Bankart lesion which is a tear of the anteroinferior labrum.
This results in instability and recurrent dislocations.
Due to these recurrent dislocations significant bone loss and erosion of the anterior glenoid rim may occur, which maintains the unstable situation.
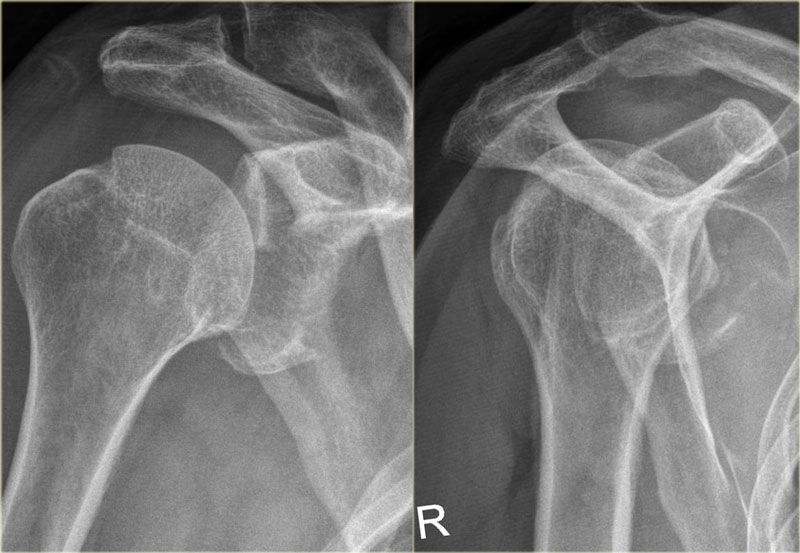
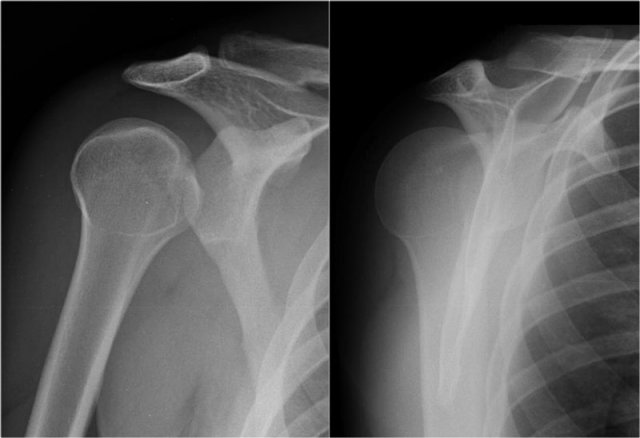
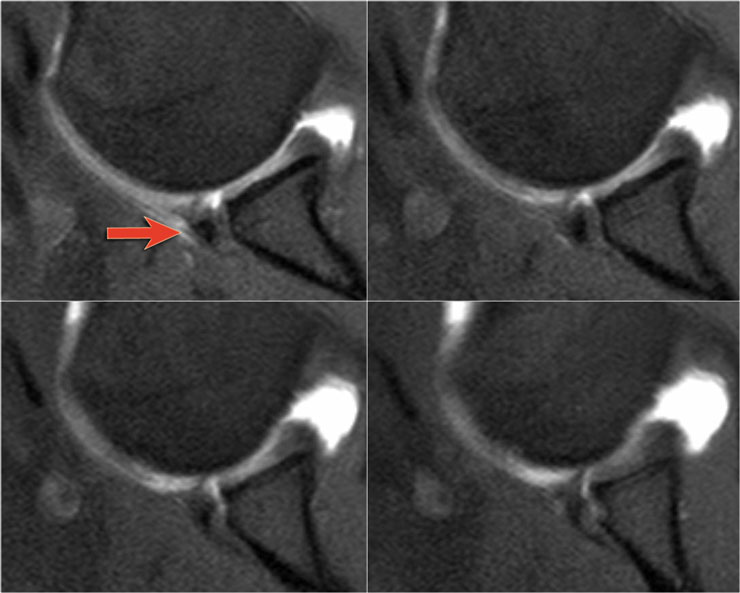
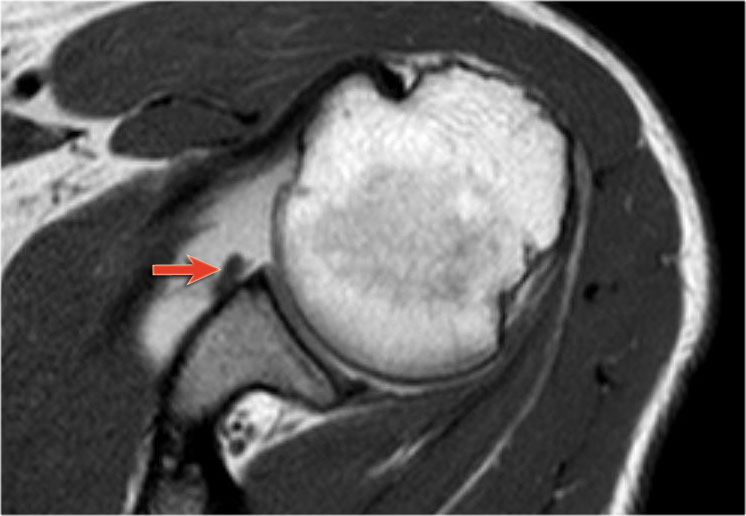
Scroll through images.

The images show a subtle Bankart fracture (arrows).
Scroll through images.
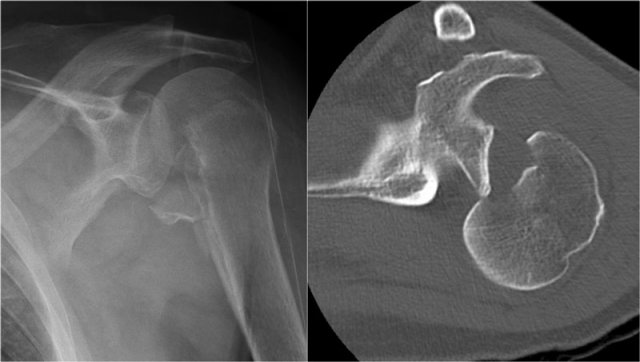
Bankart fracture
This is a post-reduction view.
Notice the very large fracture of the glenoid rim with displacement.
Scroll through images.

On the coronal-oblique and sagittal reconstruction the displaced fragment of the glenoid rim is seen in the 3-6 o'clock position.
On the coronal image a large Hill-Sachs defect is seen.
This is a bone defect as result of the impaction of the glenoid rim on the humeral head.

3D-reconstruction of a large bony Bankart in the 2 - 6 o'clock position.
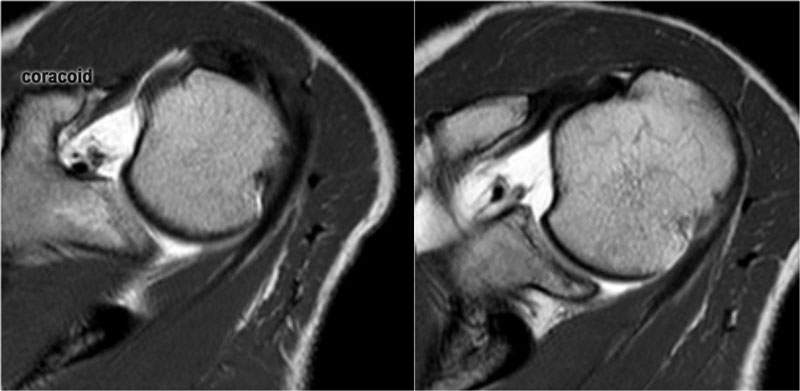
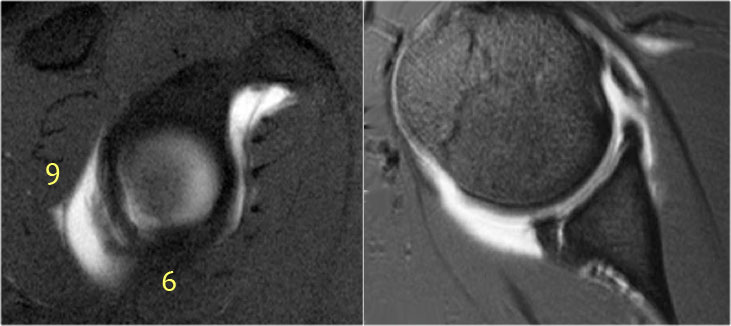
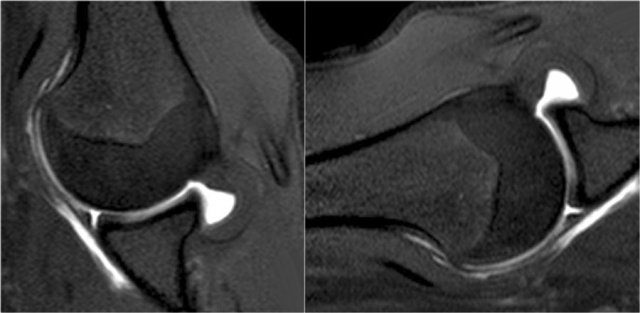
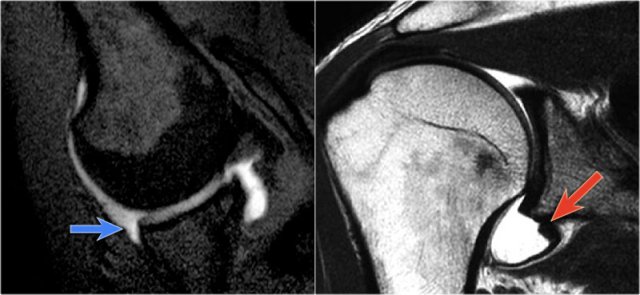
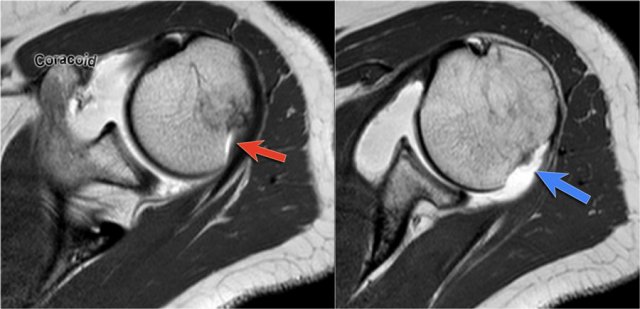 LEFT: Hill-Sachs at level of coracoid. RIGHT: Normal groove seen at level below coracoid.
LEFT: Hill-Sachs at level of coracoid. RIGHT: Normal groove seen at level below coracoid.
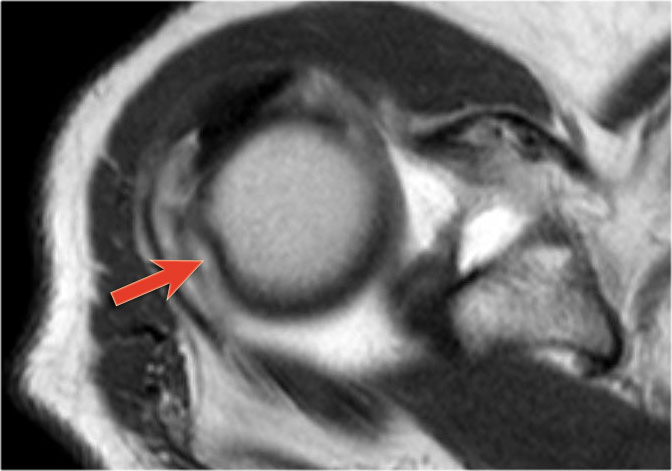
Hill-Sachs
On MR a Hill-Sachs defect is seen at or above the level of the coracoid process.
Hill-Sachs is a posterolateral depression of the humeral head.
It is above or at the level of the coracoid in the first 18 mm of the proximal humeral head.
It is seen in 75-100% of patients with anterior instability.
The physiologic groove in the humerus or cysts and erosions at the attachment site of the infraspinatus tendon can simulate a Hill-Sachs, but usually this is not a diagnostic problem (figure).
Posterior dislocation
Posterior dislocations are uncommon and easily missed, because there is less displacement compared to the anterior dislocation.
In cases of glenoid dysplasia, the posterior glenoid rim is often flattened, reducing bony stability against posterior translation of the humeral head.
This anatomical variation is more frequently associated with posterior instability and, consequently, posterior dislocations.
Images
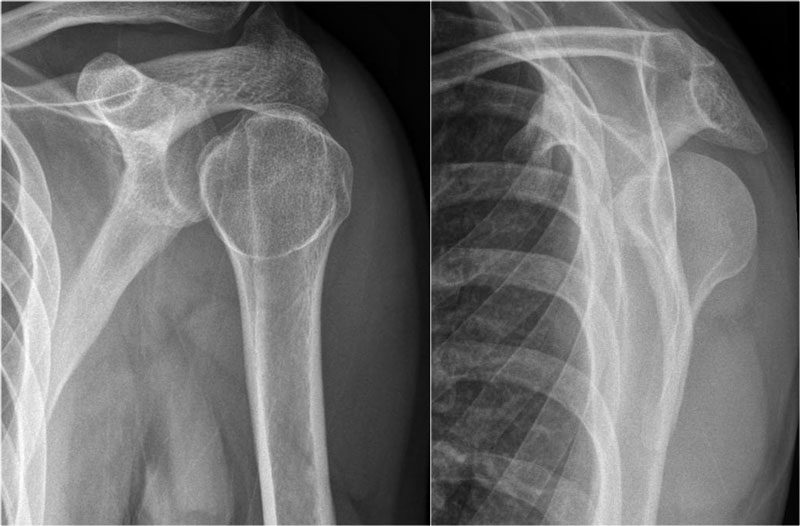
On the AP-view the head looks strange due to the internal rotation.
On the transscapular-Y view the humeral head is displaced posteriorly.
Sometimes the displacement is difficult to appreciate, especially when the transscapular-Y view is slightly rotated.
An axillary view can be helpful, but when in doubt CT is necessary.
Scroll through images.
 Posterior dislocation
Posterior dislocation
Images
- AP-view: Distance between the humeral head and the glenoid is abnormally wide.
- Transscapular-Y view: the humeral head is displaced posteriorly.
Posterior dislocations are not as obvious on the X-rays as an anterior dislocation.
Approximately half of the posterior shoulder dislocations go undiagnosed on initial presentation, because of a low level of clinical suspicion and insufficient imaging.
 Posterior dislocation-fracture
Posterior dislocation-fracture
Posterior dislocations account for 2-4% of all shoulder dislocations.
Posterior dislocations are associated with epileptic seizures, high energy trauma, electroconvulsive therapy and dysplasia of the glenoid.
On the images a posterior dislocation is seen with a fracture.
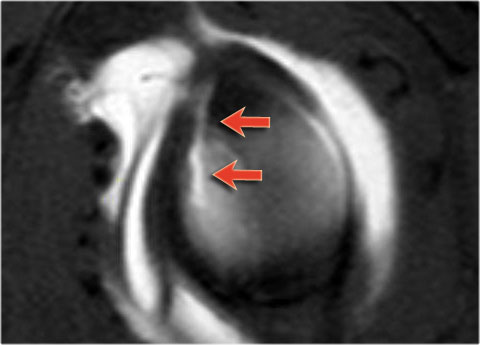
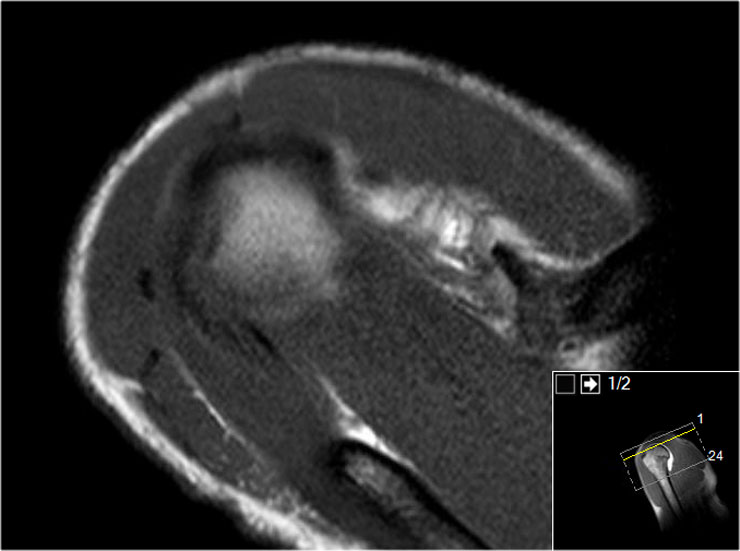
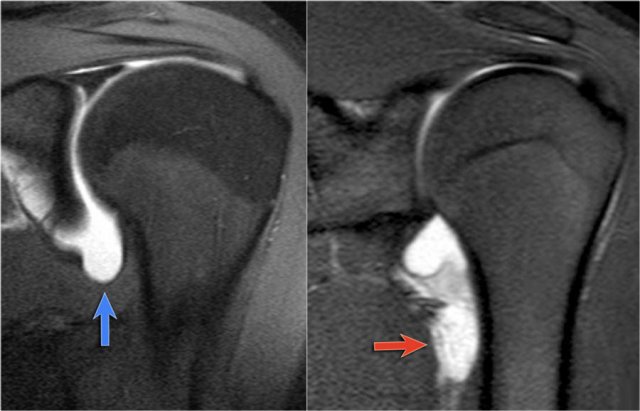
The MR-images are of a patient who had undergone both an anterior aswell as a posterior dislocation.
This resulted in both a Hill-Sachs impression fracture on the posterior aspect of the humeral head (blue arrow) and an impression fracture on the anterior aspect as a result of posterior dislocation (red arrow).
Scroll through images.
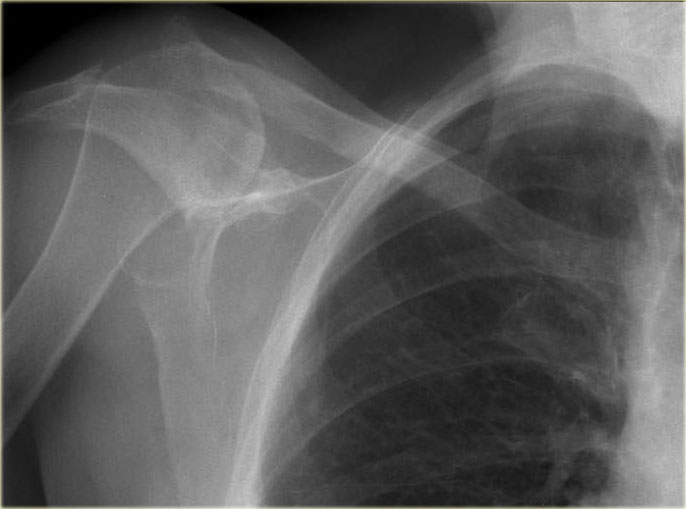 Superior dislocation
Superior dislocation
This was an incidental finding on a chest radiograph.
There is a superior dislocation of the humeral head, likely secondary to a chronic, massive rotator cuff tear.
This has resulted in progressive cranialization of the humeral head and acromial erosion.
Bankart and variants
 Axial images of Bankart lesions and variants
Axial images of Bankart lesions and variants
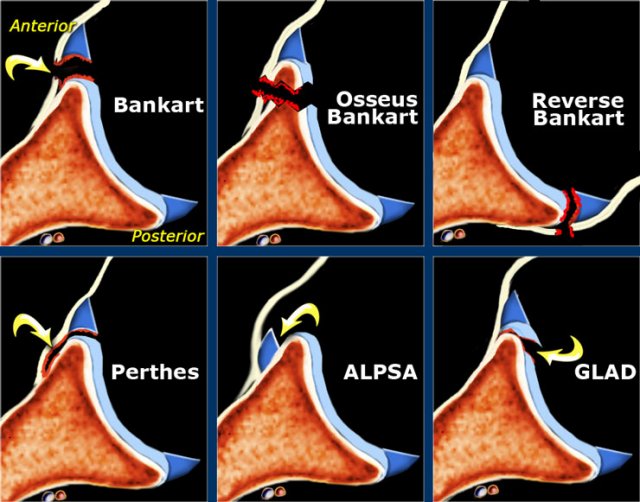
Bankart-lesions and variants like Perthes and ALPSA are injuries to the anteroinferior labrum.
These injuries are always located in the 3-6 o'clock position because they are caused by an anterior-inferior dislocation.
The only exception to this rule is the reverse Bankart, which is the result of a posterior dislocation and injury to the inferoposterior labrum.
Bankart tears may extend to superior, but this is uncommon.
- Bankart
Detachment of the anteroinferior labrum (3-6 o'clock) with complete tearing of the anterior scapular periosteum with or without an osseus fragment of the glenoid. - Reverse Bankart
Detachment of the posteroinferior labrum (6-9 o'clock) with tearing of the posterior scapular periosteum with or without an osseus fragment of the glenoid. - Perthes
Detachment of the anteroinferior labrum (3-6 o'clock) with medially stripped but intact periosteum. - ALPSA = Anterior Labral Periosteal Sleeve Avulsion.
Medially displaced labroligamentous complex with absence of the labrum on the glenoid rim. - GLAD = GlenoLabral Articular Disruption.
Represents a partial tear of anteroinferior labrum with adjacent cartilage damage.
 Bankart lesion
Bankart lesion
Bankart lesion
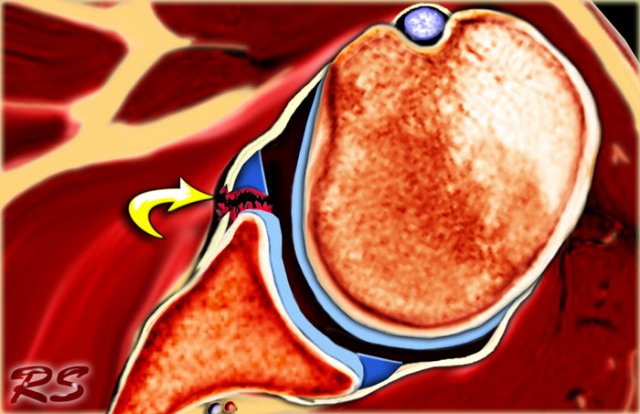
Bankart lesions are labral tears without an osseus fragment.
MR arthrography or arthroscopy are optimal to diagnose Bankart or Bankart-like lesions.
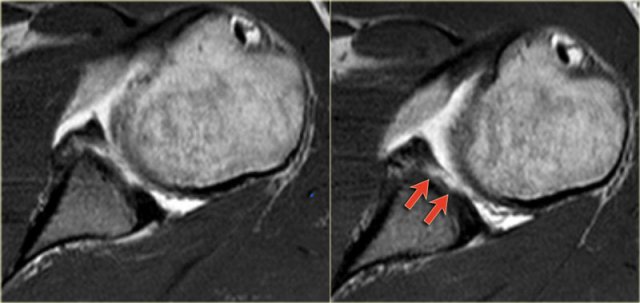
There is a detachment of the anteroinferior labrum (3-6 o'clock) with complete tearing of the anterior scapular periosteum.
The arrow points to the disrupted periosteum.

On MR-athrography the labrum is missing on the anterior glenoid and the labral fragment is displaced anteriorly (arrow).
 Osseus Bankart
Osseus Bankart
Osseus Bankart
Bankart lesions with an osseus fragment are common findings in patients with an anterior dislocation and are frequently seen on the x-rays or CT-scan.
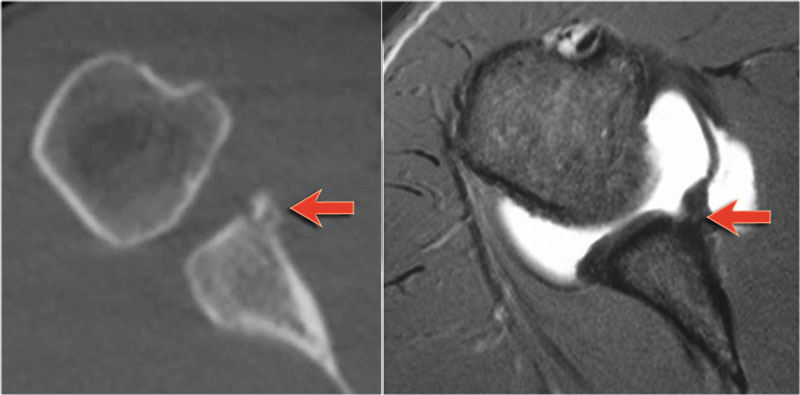 CT and MR-arthrography in a patient with an osseus Bankart (arrow)
CT and MR-arthrography in a patient with an osseus Bankart (arrow)
On MR-arthrography it may be difficult to depict the osseus fragment.
On CT it is easy to appreciate the osseus fragment of the anterior glenoid (arrow).
Scroll through the images.
There is an osseus Bankart lesion (curved red arrow).
The tear extends to superior (black arrows).
There is also a Hill-Sachs defect (red arrow).
 Bankart lesion with superior extention
Bankart lesion with superior extention
Sagittal MR-arthrogram demonstrates the superior extension of the Bankart tear.
 Osseus Bankart on a MR arthrogram ABER-view
Osseus Bankart on a MR arthrogram ABER-view
Here another patient with an osseus Bankart seen on four consecutive images of a MR arthrogram in ABER-view.
Notice the abnormal contour of the anterior glenoid and the avulsed anterior rim (arrow)

Reverse Bankart
CT-images in another patient show a reversed osseus Bankart in a patient with posterior dislocation.

Axial MR-arthrogram of a reverse Bankart.
 Reverse Bankart
Reverse Bankart
Another example of a reverse Bankart.
Notice the detatched labrum at the 6-9 o'clock position on the sagittal MR-arthrogram.
 Perthes lesion: the labrum is thorn, but the periosteum is intact and only stripped (arrow)
Perthes lesion: the labrum is thorn, but the periosteum is intact and only stripped (arrow)
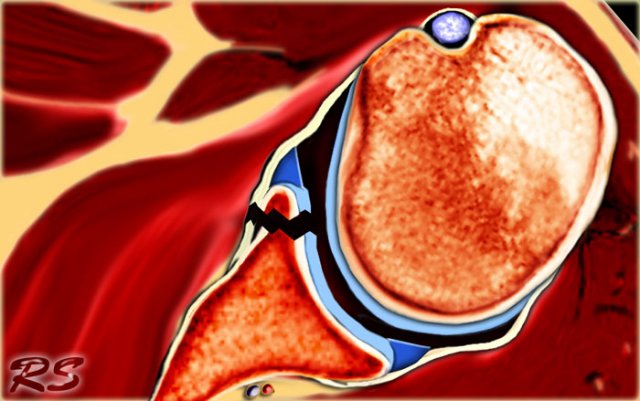
Perthes lesion
A Perthes lesion is a labroligamentous avulsion like a Bankart, but with a medially stripped intact periosteum.
On images of the shoulder with the arm in a neutral position, the torn labrum may be held in its normal anatomic position by the intact scapular periosteum, which thereby prevents contrast media from entering the tear.
This means that MR-arthrography with the arm in the neutral position may fail to detect the labral tear.
In the ABER position however there is tension on the antero-inferior labrum by the stretched anterior band of the inferior glenohumeral ligament and you have more chance to detect the tear.
The arrow points to the intact periosteum.
 LEFT: normal ABER-view. RIGHT: Image rotated 90? anti-clockwise.
LEFT: normal ABER-view. RIGHT: Image rotated 90? anti-clockwise.
The images in ABER-position demonstrate a detached anterior labrum.
The image on the right is rotated 90? anti-clockwise.
Sometimes this makes it easier to understand the anatomy.

Images of a MR-arthrogram.
The image on the left shows an absent anterosuperior labrum, which is called a Buford complex.
The image on the right shows a cartilage defect in the 4 o'clock position.
It is not clear whether the labrum is normal.
Continue with the images in ABER-position.
In the ABER-position it is obvious that there is a Perthes lesion (black arrow).
Due to the ABER-position the anterior band of the inferior GHL creates tension on the anteroinferior labrum and contrast fills the tear.
The red arrow points to the absent labrum - Buford complex.
 ALPSA.
ALPSA.
ALPSA
An ALPSA-lesion is an Anterior Labral Periosteal Sleeve Avulsion.
The anterior labrum is absent on the glenoid rim.
The arrow points to the medially displaced labroligamentous complex.
Images of a patient with an ALPSA-lesion.
Notice the medially displaced labrum.
 ALPSA-lesion
ALPSA-lesion
Images of another patient with an ALPSA-lesion.
The ABER-view shows an absent antero-inferior labrum.
The coronal images shows the medially displaced labrum (red arrow).
This is a difficult case.
First scroll through the images and try to find out what is going on.
Then continue reading.
First notice the Hill-Sachs defect indicating a prior anterior dislocation (blue arrow).
Now you know that you have to look for a Bankart or variant.
Next notice the high signal at 12 o' clock (red arrows).
On coronal images you want to make sure whether this is a variant like a labral recess or labral foramen or whether this is a SLAP.
Notice how this high signal continues posteriorly, which means that it is a SLAP-lesion.
The yellow arrow points to the anterior glenoid rim.
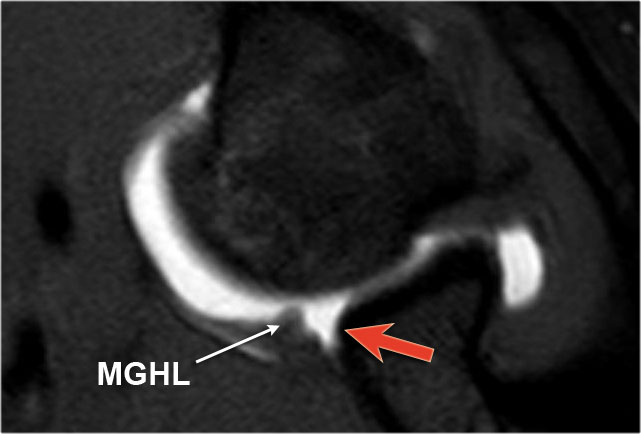
The anterior labrum is absent at the 1-3 o 'clock position
This is a Buford complex, which is a normal variant.
The structure anterior to the glenoid is not a thorn labrum, but the middle glenohumeral ligament.
Notice extention of the SLAP-tear further to posterior (red arrow).
Finally there is a medially displaced inferoanterior labrum at the 3-6 o 'clock position, i.e. an ALPSA-lesion (black arrow).
 GLAD-lesion
GLAD-lesion
GLAD
A GLAD-lesion is a GlenoLabral Articular Disruption.
It represents a patial tear of the anteroinferior labrum with adjacent cartilage damage.
The arrow points to the cartilage defect.
 GLAD-lesion
GLAD-lesion
The images show a partial tear of the anteroinferior labrum with adjacent cartilage damage at the 4-6 o 'clock position (arrows).

Scroll through the images.
There is a Bankart lesion with extension into the cartilage, i.e a GLAD-lesion (red arrows).
HAGL
 LEFT: Normal axillary recess (blue arrow). RIGHT: Abnormal axillary recess due to avulsion of the IGHL (red arrow)
LEFT: Normal axillary recess (blue arrow). RIGHT: Abnormal axillary recess due to avulsion of the IGHL (red arrow)
HAGL is a Humeral Avulsion of the inferior Glenohumeral Ligament.
There is discontinuity of the IGHL attachment on the humerus with leakage of contrast.

Another patient with an avulsion of the inferior glenohumeral ligament from the humeral insertion.