Thoracolumbar injury
Adam Flanders
Department of Radiology and Regional Spinal Cord Injury Center of the Delaware Valley, Thomas Jefferson University Hospital, Philadelphia
Publicationdate
This review is based on a presentation given by Adam Flanders and adapted for the Radiology Assistant by Robin Smithuis.
In this overview we will discuss the most common injuries of the thoracolumbar spine.
You can click on some of the images to get an enlarged view.
Introduction
Biomechanics
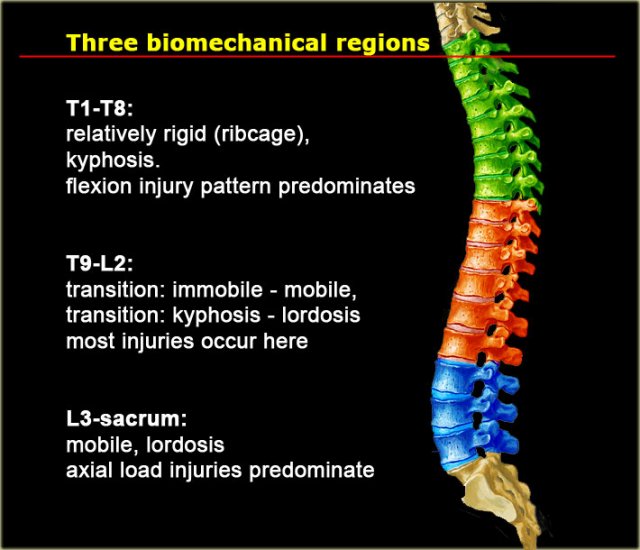
In the thoracolumbar spine there are three biomechanical regions.
The upper thoracic region (T1-T8) is rigid due to the ribcage which provides stability.
The transition zone T9-L2 is the transition between the rigid and kyphotic upper thoracic part and the flexible lordotic lumbar spine.
This is where most injuries occur.
Finally we have the L3-Sacrum zone which is flexible and this is the region where axial loading injuries occur.
 In the thoracic region flexion injuries predominate. In the lumbar region burst fractures predominate.
In the thoracic region flexion injuries predominate. In the lumbar region burst fractures predominate.
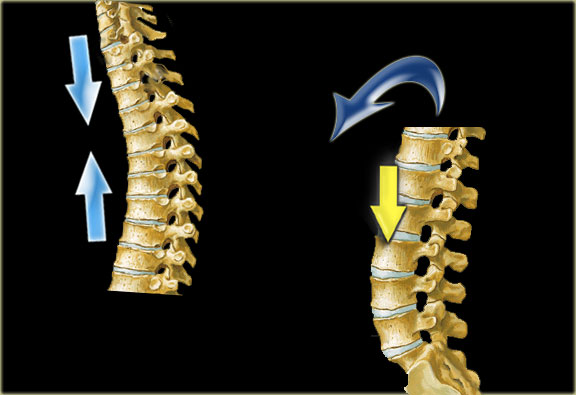
In the upper thoracic spine the center of gravity is anterior to the spine.
Axial loading will result in compressive forces anteriorly and tensile forces posteriorly.
This will result in flexion-type of injuries.
In the lumbar spine due to the lordosis, the center of gravity is posteriorly.
Flexion type of injuries will straigthen the lumbar spine and result in axial loading.
In this area we will see many burstfractures.
 Three column theory of Denis
Three column theory of Denis
Stability
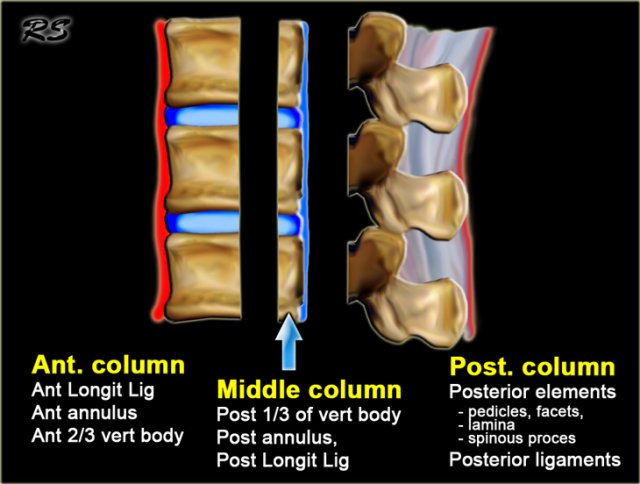
On the left the three column model of Denis.
This model is used to predict the soft tissue injury from bone injury.
Spinal stability is dependent on at least two intact columns.
When two of the three columns are disrupted, it will allow abnormal segmental motion, i.e. instability.
So a simple anterior wedge fracture or just sprain of the posterior ligaments is a stable injury.
However a wedge fracture with rupture of the interspinous ligaments is unstable, because the anterior and the posterior column are disrupted.
A burst fracture is always unstable because at least the anterior and middle column are disrupted.
Criteria to predict soft-tissue injury from bony injury are:
- Angulation greater than 20 degrees.
- Translation of 3.5 mm or more.
Hyperflexion Injury
 lwk en ct sag
lwk en ct sag
On the left images of a 31 year old male.
He was working on a roof, fell approximately 5 meters landing on his feet.
He complained of pain in left lower extremity and lower back.
First study the images, then continue reading.

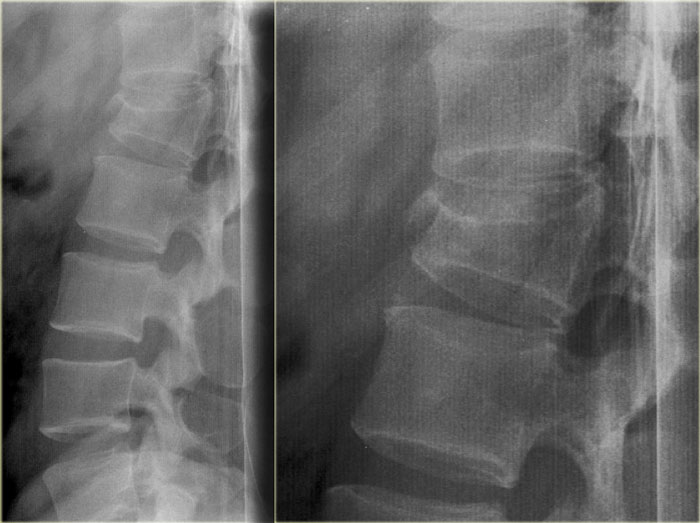
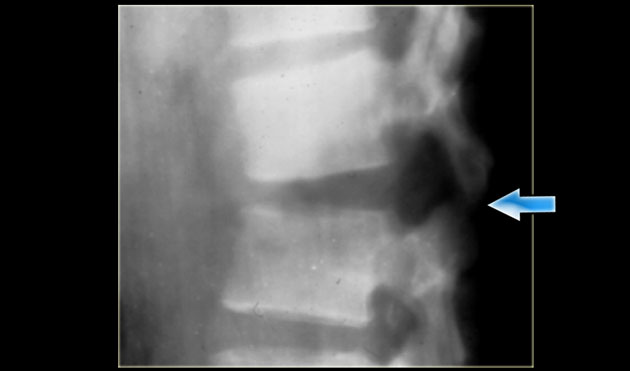
On the x-ray there is a hyperflexion injury of L1 with involvement of the anterior column and possible involvement of the middle column.
The sagittal reconstructions of the CT demonstrate that the posterior part of the vertebral body is of normal height, but there is some involvement of the posterior part of the vertebral body.
There is debate on how to treat these patients and if there is any role of MRI in these cases.
If you are aggressive you could call this a two column injury, which would require stabilizing surgery.
If you are conservative you could call this an injury with only minor involvement of the middle column.
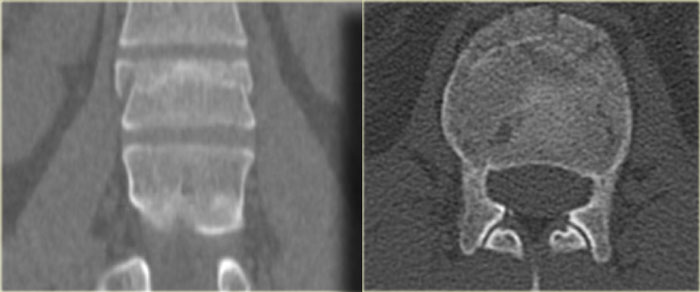
On the left a coronal reconstruction and an axial image at the level of the fracture.
Continue with the MR.
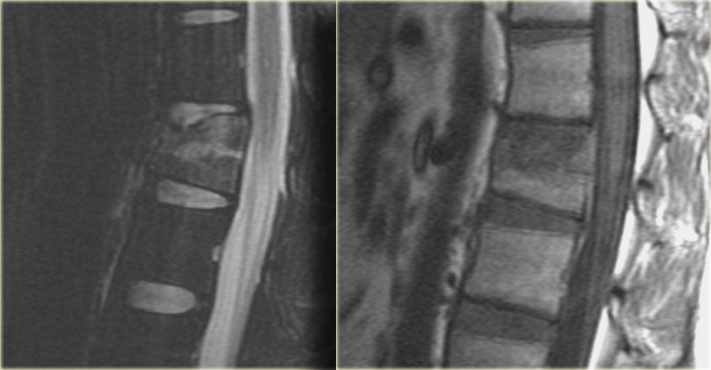 Sagittal T2WI and T1WI
Sagittal T2WI and T1WI
The MR images show bone marrow edema in the involved vertebral body, but no additional soft tissue injury.
Based on the fact that the MR did not show any additional findings, this patient was treated as having a single column injury.
Consultation with orthopedic surgery recommended conservative management with a TLSO brace.
Nowadays there is a tendency to treat these thoracolumbar injuries conservatively, even if there is slight involvement of the middle column.
The role of MRI in these cases is not clear yet.
Jumper's fracture
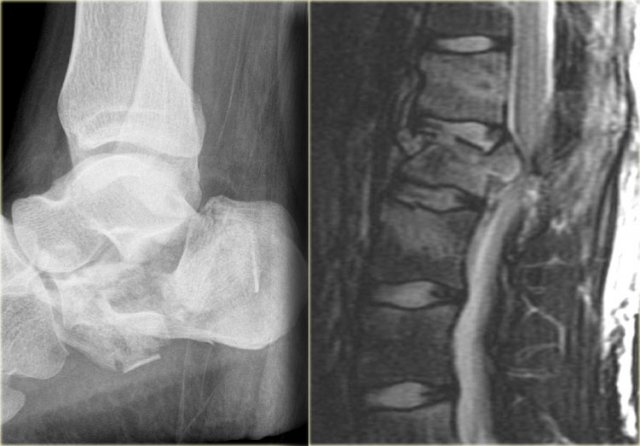
On the left a fracture of the calcaneus and a lumbar spine fracture.
This is called a 'jumpers fracture' or a 'lover's fracture', because it is usely seen in people jumping out of a window to escape from the police or a jealous husband.
In this case it is clear that we are looking at an unstable fracture, because this is a burst fracture.
Both the anterior and the middle column are disrupted.
In addition there is edema in the posterior soft tissues indicating that there is also involvement of the posterior column.
Notice also the marrow edema in the adjacent bodies due to the severe axial loading.
Chance fracture

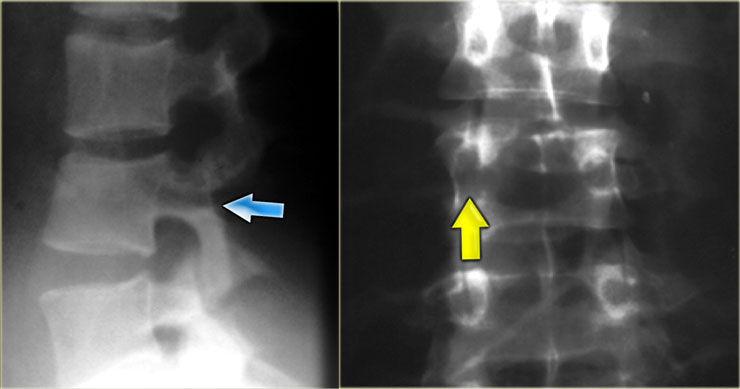
On the left images of a 21-year-old female who presented after sustaining a seatbelt type injury.
She had an exploratory laparotomy for repair of a ruptured duodenum.
There was no neurologic deficit.
First study the images, then continue reading.
What we see is a classic example of a chance fracture, which is a three column injury with a horizontal orientation of the fracture.
Continue with the CT-images.
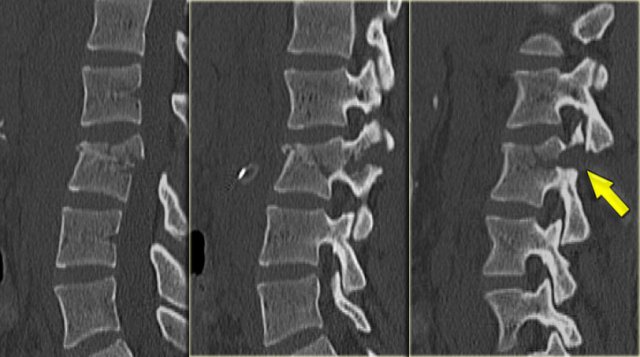
What is unique about the Chance fracture is the horizontal orientation, which is nicely demonstrated on the sagittal reconstructions on the left.
Continue with the coronal reconstructions.
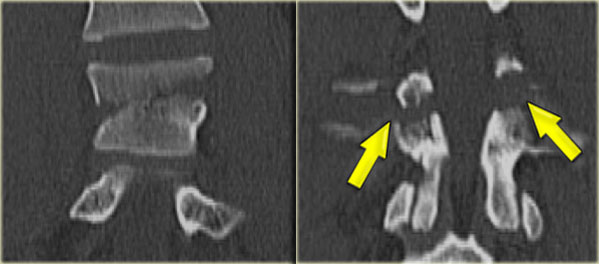
Also on the coronal reconstructions we can see the horizontal orientation of the fracture.
What type of circumstances results in a fracture of this type?
 Chance fracture due to Flexion-Distraction Mechanism.(Images courtesy of William Morrison, MD)
Chance fracture due to Flexion-Distraction Mechanism.(Images courtesy of William Morrison, MD)
The classic mechanism of this injury is a lap-belt injury.
If you don't have an addtional shoulder belt, the body will fold over.
Chance fracture (2)
On the left another example of a Chance fracture.
Chance fracture (3)
On the left a Chance variant.
This is a pure ligamentous injury, which is analogous to bilateral interfacet dislocation, which is also a pure ligamentous injury.
There is rupture of the interspinous ligament, dislocation of the facet joints and a horizontal rupture of the disc.
Pure ligamentous and combined osseous / ligamentous variants have an increased risk of instability compared to the osseus type.
Always look for a split of the posterior elements, disc widening or widening of the spinous processes and facets.