MRI examination of the ankle
Frank Smithuis and Robin Smithuis
Radiology department of the Amsterdam University Medical Centre in Amsterdam and Alrijne hospital in Leiderdorp in the Netherlands
Publicationdate
In this article a systematic approach is presented on how to describe a standard MRI of the ankle.
The following subjects will be discussed:
- Anatomy of the ankle
- Common pathology
- Variants, accessory muscles and ossicles
- MRI protocol
Systematic approach

We use a checklist when evaluating an MRI of the Ankle:
- Bones: screen on fatsat images for bone marrow edema.
- Joints: screen for effusion and look at the joint capsule for thickening.
- Ligaments: check the syndesmosis, the lateral and medial ligaments.
- Tendons: check the tendons using the four quadrant approach;
- Flexors on the medial side.
- Achilles tendon posteriorly.
- Peroneal tendons on the lateral side.
- Extensors on the anterior side.
When you have evaluated all these structures, combine your findings and try to make a specific diagnosis.
Bones

Bone marrow edema
Start your exam with fatsat images of the bones to screen for edema.
Bone marrow edema is only an indication that there is something abnormal in the bone or connected structures.
This patient has bone marrow edema on the posterior side of the distal tibia.
On the axial image, the edema is localised around the insertion site of the posterior syndesmosis.
This is edema due to a ligamentous avulsion injury.

Here two patients with bone marrow edema.
The patient on the left has bone marrow edema in the medial malleolus.
The patient on the right has edema in the medial talus.
Both patients have had an eversion injury, with stretching of the deltoid ligament.
The bone marrow edema in these patients is due to avulsion injury on the insertion sites of the deltoid ligament.

This patient has bone marrow edema in both the medial malleolus and the medial talus.
The lateral ligaments also show edema and thickening.
The bone marrow edema is likely due to impaction of talus and medial malleolus secondary to inversion injury.

Stress fractures
Stress fractures of the calcaneus are a frequently unrecognized source of heel pain.
This patient has edema in the calcaneus as a result of a stress fracture.
This injury usually results from overuse, especially in runners.
When the fracture is not seen on the T2W fatsat-images, look at the non-fatsat T2W or the T1W- images for a hypointense fracture line.

Sometimes the fracture line is not seen on MR.
In those cases you may consider a CT-scan which can be more sensitive.
This patient has multiple stress fractures of the calcaneus.

In this patient there is very subtle edema in the distal fibula.
No fracture line is visible.
There is subtle thickening of the cortex and some infiltration of the subperiosteum.
When there is edema like in this case and no visible fracture line, you may consider CT.
Do not mention the edema without having ruled out a fracture line on MR or CT.
Stress fractures are easy to miss on MR alone and this could lead to a wrong diagnosis like for instance osteomyelitis.

In this case there is a lot of edema in the navicular bone.
The axial image nicely depicts the stress fracture.

OCD
OCD is an abbreviation which can stand for either Osteochondritis Dissecans or Osteochondral Defect.
Osteochondritis dissecans is used when the patient is young and the cause is not exactly known, yet most probably due to repetitive microtrauma.
Osteochondral defect is mainly used when a patient is older or when a particular trauma is thought to be the cause of the defect.
Both describe a joint defect which involves the articular cartilage and the underlying subchondral bone.
When a small defect in the chondral plate is present, the intraarticular fluid will erode the subchondral bone, which will result in bone marrow edema.
This process can evolve into cyst formation.
Finally, when fluid flows underneath the defect, the OCD can become unstable and may result in a corpus liberum.
Here three patients with various stages of OCD.

Os Trigonum
In the foot and ankle many accessory ossicles can be seen.
The most common ossicle is the os trigonum, which is a prominent unfused apophysis of the lateral tubercle of the talus.
The os trigonum is present in the normal population in about 5-15%.

Compression of the os trigonum and surrounding soft tissues between the tibia and the calcaneus during plantar flexion can be a cause of posterior impingement.
This is especially seen in ballet dancers.
The term Stieda process is used, when the lateral tubercle is very prominent.
This can also lead to posterior impingement.

Here another patient with an os trigonum.
On the fatsat images edema is present in the os trigonum and surrounding soft tissue.
This is an example of posterior impingement due to a symptomatic os trigonum.

Here an example of an os trigonum with rather subtle edema.

This case is shown to demonstrate the great variety of ossicles and tubercles on the posterior side of the talus.
This patient has an unfused prominent lateral tubercle with a fibrous connection to the talus, therefore it is a partly fused os trigonum.
On the axial image more unfused prominent tubercles on both the medial and lateral side of the lateral tubercle are seen.
Joints

Effusion
Once you have studied the bones, scan the joints for effusion.
The left image shows a normal fluid accumulation in the tibiotalar joint, talocalcaneal joint en retrocalcaneal bursa.
The right image shows massive joint effusion as a reaction to degenerative osteochondral defects in the tibiotalar joint.
The effusion can run alongside the flexor hallucis longus tendon (FHL), since this tendon sheath is continuous with the joint.

Two examples of diffuse joint effusion in the tibiotalar joint.
There is also some joint effusion in the talocalcaneal joint.

Capsular thickening
The ankle joint is lined by the joint capsule.
When the capsule is thickened, it may cause impingement or synovitis, which can be seen in the image in the middle.
The capsule thickening can be posttraumatic or postoperative.
On the right a patient who developed postoperative fibrosis after resection of a Haglund exostosis.
There is fibrosis along the posterior calcaneus and the posterior joint capsule.

In this patient there is only a small effusion in the ankle joint.
On the non fatsat images there is subtle thickening of the capsule, with reactive changes in the surrounding soft tissue.
This patient had anterior ankle pain due to impingement by the thickened capsule.

Here another example of thickening of the capsule.
On the fatsat images, you may think that there is only some edema in the subcutaneous fatty tissue.
On the non fatsat images however, there is obvious thickened fibrotic tissue on the anterior side.
Capsular thickenig and soft tissue abnormalities are usually better seen on non-fatsat images.

In this case there is fibrous thickening of the capsule (arrow).
This patient has secundary degenerative changes in the joint with subchondral edema and cyst formation.
It is a result of repetitive impaction of the fibrotic tissue on the bone during dorsal flexion.
Ligaments

Anatomy in axial plane
Scroll through the image stack for the ligamentous anatomy in the axial plane.
You can click on the image to enlarge.
The syndesmoses are best seen on axial images:
- Anterior tibiofibular ligament or anterior syndesmosis
- Posterior tibiofibular ligament or posterior syndesmosis
- Membrana interossei, which runs all the way up to the fibular head.
The syndesmoses are usually involved in exorotation injuries like:
- Weber B fracture (Lauge Hansen Supination Exorotation injury)
- Weber C fracture (Lauge Hansen Pronation Exorotation injury)

Anterior syndesmosis
In A - a normal anterior syndesmosis is seen as a thin low intensity band.
In B - the anterior syndesmosis is thickened with edema, indicating partial tearing or grade 2 injury.
In C - the anterior syndesmosis is thickened and there probably is a focal discontinuity (arrow) and that is the reason why this was called a grade 3 injury (full thickness tear).
Isolated injury of the anterior syndesmosis can be seen in low grade exorotation injuries.

In this patient there is a full thickness tear of the anterior syndesmosis (yellow arrow).
There is also a fracture of the malleolus tertius (blue arrow).
More proximal, edema is seen around the membrana interossei.
This patient had a Weber C fracture, which is a grade 4 pronation exorotation injury in the Lauge-Hansen classification.

Posterior syndesmosis
Acute injury presents as edema and thickening, while an old injury presents with thickening and low signal intensity due to scar formation.
In A there is edema and thickening around the anterior and posterior syndesmosis (arrow), indicative of acute grade 2 injuries.
In B there is edema and thickening of the posterior syndesmosis, which is an acute grade 2 injury.
The anterior syndesmosis is also thickened but shows low signal.
This is scar formation as a result of prior injury.
In C there is scar tissue as a result of previous injury, which again can be a cause of posterior impingement.

ATFL
There are three ligaments on the lateral side:
- anterior talofibular ligament (ATFL)
- calcaneofibular ligament (CFL)
- posterior talofibular ligament (PTFL).
The ATFL runs from the lateral malleolus anteriorly to the lateral border of the talus.
It has a transverse orientation and is best seen on axial images.
This is the most commonly injured ligament of the ankle and it is also the first to be injured on the lateral side.
This means that when the CFL or the PTFL are injured, it is very likely that the ATFL is injured aswell.

Scroll through the coronal images.
You can enlarge the image by clicking on it.

Here we see three patients with ATFL injury.
The patient on the left has subtle edema around the ATFL-ligament, while the ligament itself looks normal.
This probably represents a mild strain (grade 1).
Usually this is best appreciated on fatsat images.
The patient in the middle has thickening and architecture distortion representing a partial tear (grade 2).
The patient on the right has a full thickness tear (grade 3).

Bright rim sign
This sign presents as a fine linear band of high signal intensity which is the result of a small avulsion of cortical bone in a grade 3 full thickness tear.
Here an example of a grade 3 ATFL tear with a bright rim sign (arrow).
It is thought that it is caused by a chemical shift artifact when subcortical fatty marrow is exposed to joint fluid.

CFL
The Calcaneofibular ligament runs from the distal fibula to the lateral side of the calcaneus and is best appreciated on coronal images.
The CFL passes two joints, the talocrural joint and the talocalcaneal joint.
Isolated injury of the CFL is uncommon.
Most of the time the ATFL is injured as well.

PTFL
The Posterotalofibular ligament courses posterior to the lateral tubercle on the posterior aspect of the talus.
Isolated injury is very rare.
When it is injured, there has to be injury to the other lateral ligaments.
Here a normal PTFL and a grade 2 tear.
Notice that there is also a grade 2 tear of the ATFL.

Deltoid ligament
The deltoid or medial ligament is more difficult to evaluate, since seven components have been described.
Some components are always present, while others are variable and not always seen on a standard MR.
The deltoid ligament is best evaluated in the coronal plane.
The deep layer connects the inferior border of the medial malleolus to the medial side of the talus.
The fibers are interposed with fatty tissue, giving it a striped pattern on MR.
The superficial layer of the deltoid ligament is connected to the navicular bone anteriorly and the calcaneus posteriorly.
At the insertion on the medial malleolus, it blends with the periosteum of the medial malleolus and the flexor retinaculum.
Caudally, it is connected to the Spring ligament, which is the superomedial part of the calcaneonavicular ligament.
This ligament serves as a hammock for the talus.
The Spring ligament is oriented obliquely and has a close relation with the deltoid ligament and the posterior tibial tendon.
Surgical repair of the spring ligament is increasingly being recognized as an important management component of the adult-acquired flatfoot.

These images show injury to the deep deltoid ligament.
It is difficult to differentiate between grade 1 and 2 injuries, because the edema will blur the normal striped pattern.
The image on the right shows fiber discontinuity making it a full thickness or grade 3 tear.

First look at the images.
Then continue reading.
The findings are:
- A is showing low grade injury of the deep deltoid ligament.
- B and C clearly show disruption of fibers, so these are grade 3 injuries.
- Notice additional injury to the ATFL in all cases.

On these images we can recognize the close relationship between the deltoid ligament and the periosteum of the medial malleolus and the flexor retinaculum.
On the image in the middle there is a deltoid ligament injury with separation of the periosteum or "periosteal stripping".
In addition, the flexor retinaculum is thickened.
On the image on the right there is thickening of the deltoid ligament with a low signal intensity as a result of chronic injury.
Note that the periosteum and flexor retinaculum are also thickened.
Thickening of the periosteum is a common finding and indicates injury of the deltoid ligament in the past.

Plantar fascia
The plantar fascia is a thick aponeurosis which supports the arch on the plantar side of the foot.
It runs from the tuberosity of the calcaneus to the heads of the metatarsal bones.
Plantar fasciitis, the most common cause of heel pain in the athlete, is a low-grade inflammation involving the plantar aponeurosis and the perifascial structures.
MR can show edema around the insertion of the plantar fascia on the calcaneus and spurring.
When the patient is treated, the edema will vanish, but the spurring may still be present.
Spurring as seen on a X-ray therefore can be seen in symptomatic and asymptomatic patients.
Tendons

Anatomy in the axial plane
The tendons can be divided into four compartments:
- Medial: (from medial to lateral: Tom-Dick-Harry)
- Tibialis Posterior (PTT)
- Flexor Digitorum
- Flexor Hallucis Longus
- Posterior
- Achilles
- Plantaris
- Lateral
- Peroneus Longus
- Peroneus Brevis
- Anterior (from medial to lateral: Tom-Hates-Dick)
- Tibialis Anterior
- Extensor Hallucis Longus
- Extensor Digitorum
Tendinopathy is a collective term to describe different tendon disorders like tendinosis, tendinitis and mucoid degeneration.
The pathogenesis of these disorders is different, but the clinical presentation and imaging features are not always distinctive.
Therefore it is best just to describe a tendon abnormality as tendinopathy without trying to further specifying the abnormality.
MR findings in tendinopathy are:
- Thickening
- Abnormal signal
- Tenosynovial fluid
Most tendons in the ankle joint have a tenosynovial layer.
A small amount of fluid around the tendon therefore can be normal.
The amount of fluid should not exceed the volume of the tendon itself.
The achilles tendon does not have a tenosynovial layer but a paratenon.
Fluid around the Achilles tendon is always abnormal.

Posterior tibial tendon
The posterior tibial tendon is the most commonly injured tendon.
Tendinopathy is seen as abnormal swelling of the tendon, but you have to realize, that the normal posterior tibial tendon can measure twice the size of the flexor digitorum tendon.
Posterior tibial tendon dysfunction is more common in women and in people older than 40 years of age.
It results in pain and swelling on the medial aspect of the ankle and an acquired flatfoot deformity.
Posterior tibial tendon injury in young patients is mainly due to trauma or overuse.

When the posterior tibial tendon is injured, be sure to check the spring ligmanent, since they together maintain the arch of the foot on the medial side.
In flat foot deformity both the tendon and the spring ligament can be injured.
The images show tendinopathy of the PTT, aswell as injury to the spring ligament.

Achilles tendon
The Achilles tendon is the largest and strongest tendon in the human body.
The two most common injuries are tendinopathy and rupture.
Achilles tendinopathy is most likely due to a series of microtears that weaken the tendon and cause swelling of the tendon (image on the right).

On sagital images the achilles tendon should be a straight line without any fluid around it and no focal thickening.
A transverse diameter of 8 mm is the cut off.

Three fat sat axial images of the achilles tendon.
- Left
Normal achilles tendon. Its border is concave, it is within 7mm, no paratenon fluid is seen. - Middle
Normal achilles tendon. Note that the other tendons all contain fluid, but the achilles paratenon shows no fluid at all. - Right
Fluid alongside the paratenon, i.e. paratenonitis and achilles tendinopathy.

Normally, a small amount of fluid is seen in the retrocalcanear bursa.
Too much fluid is indicative of bursitis.
Thickening of the Achilles is seen with paratenonitis.
The Haglund syndrome consists of the triad of:
- Haglunds exostosis
- Retrocalcaneal bursitis
- Achilles insertional tendinopathy
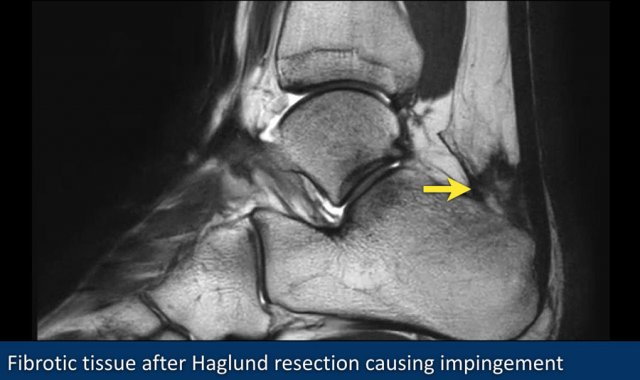
This image shows fibrotic tissue anterior to the Achilles tendon (yellow arrow) after resection of a Haglund exostosis.
This was the cause of continuing impingement.

This image shows an extreme case of insertion tendinopathy of the Achilles tendon.

Another example of Achilles tendinopathy.

Rupture of the Achilles tendon usually occurs in the part of the tendon situated within 6 centimeters of the insertion to the calcaneus.
This part is prone to rupture because the blood flow in this area is poor, which also can impair its ability to heal.
The image shows an old rupture.

Peroneal tendons
The peroneus brevis tendon is injury-prone, because it is positioned inbetween the fibula and peroneus longus tendon.
As the foot undergoes dorsiflexion, the peroneus brevis tendon is repeatedly compressed between the peroneus longus tendon and the lateral malleolus, predisposing to tear.
Once a small tear is initiated, it will results in a cashew nut deformity.
The peroneus longus tendon migrates forward into the peroneus brevis tendon tear, thereby preventing healing (figure).

In the middle and right we see two examples of cashew nut deformity, indicative of partial split rupture.
This can be challenging, because the actual tear cannot be seen, only the architectural deformation.

Split tears are associated with inversion injuries, most likely due to greater force on these tendons after ligamentous injury.
Split tears of the peroneus longus are less common.
They are associated with a prominent calcaneal tubercle.
Anterior
The extensor tendons are rarely injured.
Tom Hates Dick is a useful mnemonic.
Accessory muscles

Accessory muscles are frequently seen around the ankle joint.
Since they have a normal signal intensity, they are easily missed.
However when you compare the findings with the normal patient on the left, you will detect the big accessory soleus muscle.

Some examples of accessory muscles.
They are usually asymptomatic, but can be a cause of impingement in specific patient groups (dancers, athletes).
Accessory FHL or FDL are associated with tarsal tunnel syndrome.

The patient on the right has a hypertrophic plantaris muscle.
This can be a cause of Achilles tendinopathy.
MRI protocol

Standard axial, coronal and sagittal planes are used in the ankle both on 1.5T and in 3T.
In addition to the standard planes, a oblique scan is sometimes included oriented perpendicular to the peroneus and tibialis posterior tendons.
Small tears or subtle tendinopathy are better visualized on these views.
The orientation of the tendons along the medial and lateral malleolus can cause the 'magic angle artifact' to occur.
The tendons will show relatively hyperintense signal at 55* to B0), simulating pathology like tendinopathy or partial tears.
This artifact is visible on short TE images (f.e. PD).
On long TE images (like T2) this artifact does also occur but less pronounced.